Download
1 / 1
10 likes | 159 Views
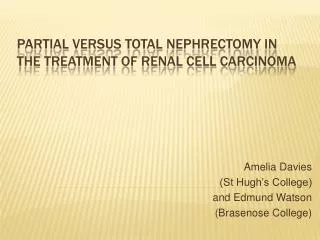
Non-neoplastic renal parenchyma. Tumor. 2. 3. 1. 1. 3. 3. 3. 3. 3. 1. 1. 2. 2. 2. 1. 3. 2. 2. 1. 3. 1. 2. 3. Poster ID:1106. Viability of glomeruli adjacent to tumor in partial nephrectomy specimens for renal cell carcinoma.

E N D
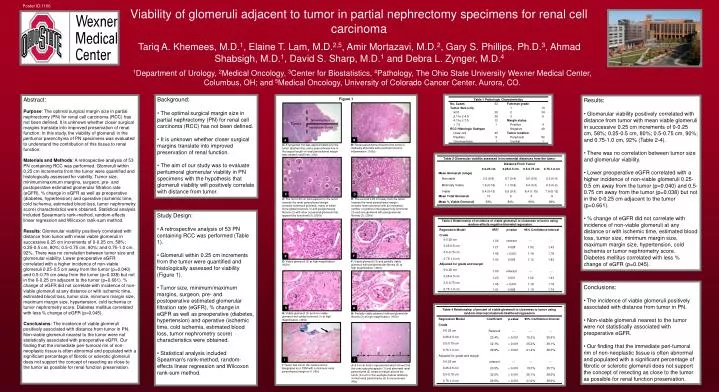
Non-neoplastic renal parenchyma Tumor 2 3 1 1 3 3 3 3 3 1 1 2 2 2 1 3 2 2 1 3 1 2 3 Poster ID:1106 Viability of glomeruli adjacent to tumor in partial nephrectomy specimens for renal cell carcinoma Tariq A. Khemees, M.D.1, Elaine T. Lam, M.D.2,5,Amir Mortazavi, M.D.2, Gary S. Phillips, Ph.D.3, Ahmad Shabsigh, M.D.1, David S. Sharp, M.D.1 and Debra L. Zynger, M.D.4 1Department of Urology, 2Medical Oncology, 3Center for Biostatistics, 4Pathology, The Ohio State University Wexner Medical Center, Columbus, OH; and 5Medical Oncology, University of Colorado Cancer Center, Aurora, CO. • Background: • The optimal surgical margin size in partial nephrectomy (PN) for renal cell carcinoma (RCC) has not been defined. • It is unknown whether closer surgical margins translate into improved preservation of renal function. • The aim of our study was to evaluate peritumoral glomerular viability in PN specimens with the hypothesis that glomeruli viability will positively correlate with distance from tumor. Abstract: Purpose: The optimal surgical margin size in partial nephrectomy (PN) for renal cell carcinoma (RCC) has not been defined. It is unknown whether closer surgical margins translate into improved preservation of renal function. In this study, the viability of glomeruli in the peritumor parenchyma of PN specimens was evaluated to understand the contribution of this tissue to renal function. Materials and Methods: A retrospective analysis of 53 PN containing RCC was performed. Glomeruli within 0.25 cm increments from the tumor were quantified and histologically assessed for viability. Tumor size, minimum/maximum margins, surgeon, pre- and postoperative estimated glomerular filtration rate (eGFR), % change in eGFR as well as preoperative (diabetes, hypertension) and operative (ischemic time, cold ischemia, estimated blood loss, tumor nephrometry score) characteristics were obtained. Statistical analysis included Spearman's rank-method, random-effects linear regression and Wilcoxon rank-sum method. Results: Glomerular viability positively correlated with distance from tumor with mean viable glomeruli in successive 0.25 cm increments of 0-0.25 cm, 58%; 0.25-0.5 cm, 80%; 0.5-0.75 cm, 90%; and 0.75-1.0 cm, 92%. There was no correlation between tumor size and glomerular viability. Lower preoperative eGFR correlated with a higher incidence of non-viable glomeruli 0.25-0.5 cm away from the tumor (p=0.040) and 0.5-0.75 cm away from the tumor (p=0.038) but not in the 0-0.25 cm adjacent to the tumor (p=0.661).% change of eGFR did not correlate with incidence of non-viable glomeruli at any distance or with ischemic time, estimated blood loss, tumor size, minimum margin size, maximum margin size, hypertension, cold ischemia or tumor nephrometry score. Diabetes mellitus correlated with less % change of eGFR (p=0.045). Conclusions: The incidence of viable glomeruli positively associated with distance from tumor in PN. Non-viable glomeruli nearest to the tumor were not statistically associated with preoperative eGFR. Our finding that the immediate peri-tumoral rim of non-neoplastic tissue is often abnormal and populated with a significant percentage of fibrotic or sclerotic glomeruli does not support the concept of resecting as close to the tumor as possible for renal function preservation. • Results: • Glomerular viability positively correlated with distance from tumor with mean viable glomeruli in successive 0.25 cm increments of 0-0.25 cm, 58%; 0.25-0.5 cm, 80%; 0.5-0.75 cm, 90%; and 0.75-1.0 cm, 92% (Table 2-4). • There was no correlation between tumor size and glomerular viability. • Lower preoperative eGFR correlated with a higher incidence of non-viable glomeruli 0.25-0.5 cm away from the tumor (p=0.040) and 0.5-0.75 cm away from the tumor (p=0.038) but not in the 0-0.25 cm adjacent to the tumor (p=0.661). • % change of eGFR did not correlate with incidence of non-viable glomeruli at any distance or with ischemic time, estimated blood loss, tumor size, minimum margin size, maximum margin size, hypertension, cold ischemia or tumor nephrometry score. Diabetes mellitus correlated with less % change of eGFR (p=0.045). Figure 1 B A B: Renal parenchyma closest to the tumor is markedly abnormal with prominent chronic inflammation. (100x) A: A tangential line was approximated over the tumor (dashed line) and a perpendicular line to the largest length of renal parenchymal margin was created (solid line). (40x) C D C: The first 0.25 cm field adjacent to the tumor towards the renal parenchymal margin contains numerous glomeruli, many of which show global sclerosis (1) and periglomerular fibrosis (2) with other occasional glomeruli that appear fully functional (3). (200x) D: The second 0.25 cm away from the tumor towards the renal parenchymal margin contains fewer glomeruli with an increased number of glomeruli that appear fully functional (3) and rare glomeruli with periglomerular fibrosis (2). (200x) • Study Design: • A retrospective analysis of 53 PN containing RCC was performed (Table 1). • Glomeruli within 0.25 cm increments from the tumor were quantified and histologically assessed for viability (Figure 1). • Tumor size, minimum/maximum margins, surgeon, pre- and postoperative estimated glomerular filtration rate (eGFR), % change in eGFR as well as preoperative (diabetes, hypertension) and operative (ischemic time, cold ischemia, estimated blood loss, tumor nephrometry score) characteristics were obtained. • Statistical analysis included Spearman's rank-method, random-effects linear regression and Wilcoxon rank-sum method. 3 2 F E F: Viable glomeruli (3) and partially viable glomeruli with periglomerular fibrosis (2) at high magnification. (400x) E: Viable glomeruli (3) at high magnification. (400x) • Conclusions: • The incidence of viable glomeruli positively associated with distance from tumor in PN. • Non-viable glomeruli nearest to the tumor were not statistically associated with preoperative eGFR. • Our finding that the immediate peri-tumoral rim of non-neoplastic tissue is often abnormal and populated with a significant percentage of fibrotic or sclerotic glomeruli does not support the concept of resecting as close to the tumor as possible for renal function preservation. G H G: Viable glomeruli (3) and non-viable glomeruli with global sclerosis (1) at high magnification. (400x) H: Partially-viable glomeruli with periglomerular fibrosis (2) at high magnification. (400x) J I I: Tumor has ink on the surface and is designated as a PSM with a minimum renal parenchymal margin of 0. (40x) J: A 0.6 cm field is represented which shows that the tumor pseudocapsule (1) and abnormal renal parenchyma (2) create a margin around the tumor (0.4 cm in this example) before relatively normal renal parenchyma (3) is encountered. (40x)