Download
1 / 16
160 likes | 279 Views
Identify the Ways to Increase Access of FP Services in Hard to Reach Areas and Urban Slums. Dr. Kazi Maruful Islam Eminence 3/6, Asad Avenue, Mohammadpur Dhaka- 1207. Objectives. Identify the constraints to increase FP users in hard to reach area and urban slums

E N D
Identify the Ways to Increase Access of FP Services in Hard to Reach Areas and Urban Slums Dr. KaziMaruful Islam Eminence 3/6, Asad Avenue, Mohammadpur Dhaka- 1207.
Objectives • Identify the constraints to increase FPusers in hard to reach area and urban slums • Define the factors that differentiate urban slum women in accessing FP services compared to hard to reach areas of rural women • Find out means of reaching the FP services in hard to reach and urban slum areas
Methodology • Methods used • Quantitative • Survey with structured questionnaire with 1500 married women at reproductive age (Rural 700 and Urban 800) • Qualitative • Document Review (Relevant documents and web portal) • Focused Group Discussion (14 groups) • Key Informant Interview (42 KII with government health service providers, pharmacy manager in urban areas, religious leaders and community leaders) • -
Methodology • Study areas • Hard to reach areas in 7 Administrative divisions and urban slums of City Corporations • Barisal:Barishal CC and Bhola • Chittagong: Chittagong CC and Banderban • Dhaka: Dhaka CCs and Jamalpur Char • Khulna: Knulna CC and Satkhira • Rajshahi: Rajshahi CC and Baghmara • Rangpur: RangpurSadar and Ganchhara • Sylhet: Sylhet CC and Habiganj
Obj-1: Constraints in providing FP Services in Hard to Reach areas and Urban Slums Hard to Reach Areas Demand Side Desire for more children (34.2%) Denial of women (23.1%) Husband’s denial/opposition (28.3%) Religious barrier/misconceptions (15.3%) Supply Side Shortage of FP field workers Lack of training and motivation of field workers Communication and transport difficulty of field workers Location of Community clinics Unavailability of contraceptives as per demand and suitability.
Obj-1: Constraints in providing FP Services in Hard to Reach areas Urban Slums Demand Side Desire for more children (37.8%) Denial of women (18.9%) Husband’s denial/opposition (21.3%) Religious barrier (3.3%). Supply Side Absence of government FP workers Unavailability of contraceptives as per demand and suitability.
Obj-2: Differentiating factors of Hard to reach areas and Urban slums in accessing to FP Services Population density: Less in hard to reach than urban slums Availability of family planning services: Government workers in hard to reach areas; not in urban slums, only pharmacy and NGO workers Accessibility and affordability: Service is physically inaccessible in hard to reach areas, not depends much on even affordability; Hospitals and pharmacies are accessible in urban slums Religious and cultural barrier: Less in urban slums
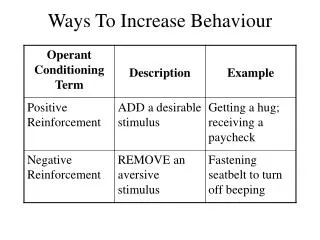
Obj-3: Means of reaching FP services • Hard to Reach Areas • Increase household visit of field workers (50.2%) • Provision of alternative oral pills (26%) • Correct advice from service providers (21.4%) • Rigorous campaign and target male members of the • family/husband (Qualitative methods) • Urban Slums • Provision of alternative short term methods (16.6%) • Correct advice from service providers (19.1%) • Alternatives for long term and permanent methods (24.2%) • Provision of government family planning workers (24%) • Frequent visit of FP workers according to clients’ time (12.1%)
LESSON LEARNT • In hard to reach areas community clinics/health complexes are sometimes physically inaccessible. • Communities are not informed properly about the revised schedule of FP worker (e.g. FP workers are available in community clinics 3 days/week) • Misconception about the government provided brands of FP method
LESSON LEARNT • Clients discontinue methods because of unavailability of their preferred methods/brands • Mismatch of timing between eligible couples in urban slums and health service providers. • Males are less involved in in decision making, acceptance, and use of family planning • Religious misconceptions higher in hard to reach areas
RECOMMENDATIONS • Special and organized drive to make FP services accessible and available in hard to reach areas • Policy level decision on placement of field workers • Introduction of systematic screening to identify individual suitability of the contraceptive methods
RECOMMENDATIONS • Sensitization and motivation of eligible couples , religious leaders, LGI representatives and others through innovative ways of information dissemination and health education (e.g mobile based technology, khutba at weekly prayer etc) • Encourage male participation in family planning and couple’s reproductive health