Download
1 / 15
150 likes | 295 Views
Molecular Analysis of B cell Subsets in Common Variable Immunodeficiency (CVID). A Ridley , S Harris, J Burden, B Ferry, A Janda, Z Davis, D Oscier, AP Williams, JL Smith, E Hodges. CVID. 1 in 50,000 Most common primary antibody deficiency Diagnosed between 20 & 40 years

E N D
Molecular Analysis of B cell Subsets in Common Variable Immunodeficiency (CVID) A Ridley, S Harris, J Burden, B Ferry, A Janda, Z Davis, D Oscier, AP Williams, JL Smith, E Hodges
CVID • 1 in 50,000 • Most common primary antibody deficiency • Diagnosed between 20 & 40 years • Heterogeneous syndrome • Decreased Ig levels • Recurrent infections • Other causes of immunodeficiency excluded
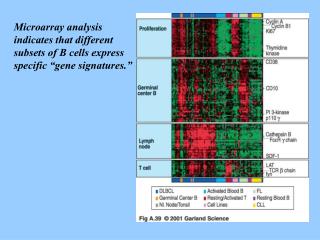
naive memory IgM Memory ~20% Ig M/D Class Switched Memory ~20% CD27 naive memory IgM Memory ~4% Ig M/D Class Switched Memory ~1% CD27 naive memory IgM Memory ~20% Ig M/D Class Switched Memory ~4% CD27 Classification of CVID LPD Granulomatous Splenomegaly MB0 Reduced memory B cells MB1 Reduced class switched memory B cells Splenomegaly MB2 Class switched memory B cells Clinical complications less severe
IgD+/CD27+ • IgD-/CD27+ Somatic hypermutation (SHM): nucleotide substitution in V region to increase affinity for antigen Class switch recombination (CSR): B-cells substitutes expression of IgM and IgD for IgG, IgA or IgE by deleting DNA between switch regions IgD+ and CD27-
Aim • Molecular methodology to develop CVID classification to a molecular level • Investigation of the pattern and frequency of somatic hypermutation in B cell subgroups as defined by CD27 expression • Restriction enzyme-based hot-spot mutation assay (REHMA): screening test to detect the presence of SHM in B cells of CVID patients • To allow improved characterisation, prognosis and management of CVID patients
3 CLL patients • 9 healthy controls • 10 CVID patients Flow cytometric analysis of B cells using CD19/IgM /IgD/CD27 antibodies Separation of CD27+ peripheral blood B cells Extract RNA & set up RT-PCR reactions to obtain cDNA • Amplification with: • IgGVH3-23 and C • FR1 and FR3 primers Cloning & sequencing of PCR products to identify the pattern of somatic hypermutation RE digestion & fragment length analysis by capillary electrophoresis Correlate levels of somatic hypermutation to previous phenotypic classification
IgVH3-23 Cγ FR1 FR3 Ser31 Ser35 Ala50 202 bp 119 bp Alu I 158 bp 164 bp Alu I 175 bp Alu I Ig Heavy Chain SHM Analysis Specific product 202 bp 2nd round PCR product Mutated 202 bp Ava II Alu I RE digest Unmutated 164 bp 119 bp 175 bp 202 bp Alu I RE digest
Ava II 1 158 bp 119bp Alu I 2 Ava II 158 bp 3 158 bp Ava II 164 bp 164 bp Alu I Alu I RE digestion of CLL patients Ser35 Ala50 Ser31 Hot spots
Specific product 202 bp Ava II 158 bp 119 bp 164 bp 175 bp 202 bp Alu I Ser35 Ser31 Ala50 Hot spots RE digestion of a healthy control
119bp 164 bp Control 175bp 202 bp CVID 1 Ser35 Ser31 Ala50 Hot spots Alu1 digestion of MB0 CVID patients CVID 2 CVID 3
164 bp 119 bp 175 bp Control 202 bp CVID 4 CVID 5 CVID 6 CVID 7 CVID 8 Alu1 digestion of MB1 CVID patients Ser35 Ser31 Ala50 Hot spots
164 bp Control 119 bp 175 bp 202 bp CVID 9 CVID 10 Ser35 Ser31 Ala50 Hot spots Alu1 digestion of MB2 CVID patients
Mutational status by sequence analysis Percentages of sequences with 0-1, 2-10, 11-20 and 21-30 mutations from a healthy control, an MB2 patient & an MB1 patient
Summary • Rapid, non-radioactive screening method to look at SHM in CVID • REHMA confirmed by sequence analysis • REHMA patterns heterogeneous in the CVID subgroups defined by phenotype • Correlation to clinical disease • Investigation of IgM IgVH3-23 transcripts • Use of PBMC
SGH, Immunology & Molecular Pathology Dr E Hodges Dr J Smith S Harris A Williams Z Shah Churchill Hospital, Oxford J Burden Dr B Ferry Dr A Janda Royal Bournemouth Hospital Dr D Oscier Z Davis Acknowledgments