Download
1 / 30
310 likes | 510 Views
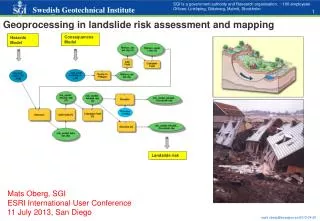
Risk assessment tools in intra-partum care: intended and unintended consequences SDHI Conference, St Andrews, Scotland. Nicola Mackintosh, Jane Sandall 27 June 2011. Research Context. Context: Innovations Programme / NIHR King’s PSSQ Research Centre

E N D
Risk assessment tools in intra-partum care: intended and unintended consequencesSDHI Conference, St Andrews, Scotland Nicola Mackintosh, Jane Sandall 27 June 2011
Research Context Context: Innovations Programme / NIHR King’s PSSQ Research Centre • The Innovations Programme looks at both the translation of novel technologies into health care and innovative ways of organising services differently to bridge ‘gaps’ in care and improve quality and safety for patients This Project: • two year study examining the management of complications in medicine and maternity
Outline Background - Policy context / Clinical context / Theory Findings - implementation of early warning systems in maternity settings The tool in-action; intended and unintended consequences The tool doesn’t fit here The tool’s role in women’s journeys through care; a help and a hindrance Rational workarounds Questions / discussion - feeding back results regarding the ‘bright’ and ‘dark’ side of organisational work Research priorities
Policy context Healthcare reconceived as a ‘system’, transformation of the current culture of blame into a culture of safety Focus on prediction, control & avoidance ‘System theoretical approach has become a leverage point for imagining interventions in healthcare’ (Jenson 2007) Reductions in risks associated with social activities e.g. quantification of accurate scientific information (Gabe 1995) plus the ‘technological fix’ (Stabile 1994)
Clinical context – maternity care • Characterised by medicalisation, institutionalisation, risk & bureaucratisation (Walsh 2010) • ‘High stake’ setting • Plethora of expert views • Regulation of decision making & support for technological interventions (Lankshear 2005)
Clinical context - the ‘problem’ For the most part, pregnancy and birth is a normal physiological process, but emergencies can develop rapidly and unexpectedly Potential for poor outcomes for mother and/or the baby Substandard care in 70% of the direct, 55% of the indirect maternal deaths Many of the identified avoidable factors remained the same as those identified in previous Enquiries (CMACE 2011) Women’s experiences of birth trauma - poor communication, diminished agency, insensitive care (Beck 2006)
Clinical context - ‘Failure to rescue’ • The terms is used across all clinical specialties • Additional complexities within maternity • The space between physiology and pathology • The relative rarity of such events
Clinical context - proposed solution “There is an urgent need for the routine use of a national obstetric early warning chart, similar to those in use in other areas of clinical practice, which can be used for all obstetric women which will help in the more timely recognition, treatment and referral of women who have, or are developing, a critical illness”. CEMACE, Saving Mothers’ Lives 2003-2005
Evidence Base Poor methodology & wide variations between different systems restrict comparison of outcomes and standardisation (Gao et al., 2007; McGaughey et al., 2007).
Theory - organisational cultural theory • Drawing on Vaughan’s organisational cultural theory - the normal, rational and functional aspects of organisations can also produce a ‘dark side’ • The same organisational cultural processes that promote normal functioning, e.g. routines, rules of thumb, and institutional understandings can also create mistakes
Theory – the ‘Bright’ or the ‘Dark’ side? • Training, often used to prevent errors, can create them; information richness introduces inefficiency, too little produces inaccuracy; teams have multiple points of view that enhance safety, but as they become a cohesive group they share assumptions, so the “requisite variety” important to safety is lost (Vaughan 1999: 297)
Theory - analyses of socio-technical systems: Environment Organisation characteristics (structure, process, tasks) Cognitive practices
PSSQ research: Managing complications in maternity Aim: To explore the management of intra-partum complications and escalation of care Data collection: March 2010 to Jan 2011 Two UK Trusts Ethnographic methods: Documentary analysis Observation of meetings, ward life and key events (>120 hours) Audio-recorded interviews: 44 interviews with staff and external stakeholders, postnatal women and some partners [21] NVivo coding and analysis of fieldnotes and interview transcripts
Findings – the themes • The tool in-action; intended and unintended consequences • The tool doesn’t fit here • The tool’s role in women’s journeys through care; a help and a hindrance • Rational workarounds
Findings: intended consequences • ‘they raise awareness of these observations, people speak in terms of thresholds and everyone knows what’s abnormal. People used to say, ‘Somebody’s breathless,’ but now the midwife will be able to say, ‘She’s breathless and her respiratory rate is 40,’ which automatically rings bells’ (Site B, Obstetrician) • ‘although you can say, ‘if the midwife sees the patient’s breathing fast she can come and get us, can’t she?’ I’m aware a lot of midwives feel quite apprehensive about coming along with one sign they’re not really sure of the significance of. If they’re empowered to come and … get somebody, then that’s useful (Site B, Anaesthetist)
Findings: unintended consequences Privileging some actors / voices and marginalising others • A new admission has been referred by a community midwife, with a blood pressure of 130/80, which according to the community midwife is very abnormal for her. Her booking blood pressure had been about 100 systolic, so the community team feel this is a significant increase. She also has a trace of protein in her urine and slight oedema. The medical team note ‘this isn’t high blood pressure’, ‘the fact that her booking blood pressure was lower than that is ‘insignificant’.’(Field notes, Site B)
Findings: the tool doesn’t fit here • ‘the general Trust EWS doesn’t fit maternity and doesn’t fit children’s services, so those areas have developed their own [tools], but perhaps not with support from the rest of the Trust to make sure they’re really robust, and that’s the bit that I feel is a bit difficult [..] I think sometimes [..] we’re just a little bit in that too difficult box. [Laughs] so you just do your own thing!’ (Site A, Manager)
Findings: the tool doesn’t fit here • The risk manager reports that a recurring problem is poor documentation, observations not recorded and half hourly maternal pulse not checked during labour. She says that a random spot check done in June 2009 found that half hourly maternal pulse wasn’t recorded in any of the selected sets of notes. She feels it’s improved since then but she’s also aware that this is one of the major issues in some of the incident forms that are flagged up (Site B, Field notes)
Findings – helping and hindering women’s journeys through care
Findings: helping women’s journeys through care • When S, the consultant obstetrician, comes on this morning she queries why one woman is still on the unit, she suggests she could go to the post-natal ward. Yet when S looks through her notes she finds it difficult to get an overview of the woman’s progress. Because the midwives haven’t been using a MEOWS chart, choosing to write the observations in the notes instead, she asks a house officer to plot the temperature manually and sees there is a very slow upward trend. She then reverses her decision and decides this woman needs to stay on the unit (Site B, Field notes)
Findings: helping and hindering women’s journeys through care • I ask the consultant what she feels the issues are on the unit in terms of facilitating or impeding the process of escalation of care for acutely ill women. She reports the problem isn’t necessarily capacity or lack of beds on the unit, it is more about flow through the unit. She notes blockages at exit points (e.g. the postnatal ward) which creates a sense of a ‘traffic jam’ on the unit (Field notes, Site B)
Findings: rational workarounds • ‘I’ve started running away from [the Hypertension Consultant] because I know what he’s going to say to me. He’s going to speak to me about these MEOWS charts … at the moment the healthcare assistants tend to write the observations on a piece of paper, they give it to the midwives, the midwives will have looked at them and put them in her pocket, he’s really stressing because they’re not on the chart … I appreciate what he’s saying, why can’t the midwives do it, it only takes two minutes to write something on a chart. Yeah it only takes two minutes but they’ve got ten women to look after, that’s ten sets of observations. They’ve also got to arrange their tablets, arrange the discharge, labour wards are calling for beds, we’ve got a baby that is jaundiced, each thing individually sounds easy but in realistic terms, with the whole scope of things, it’s not that manageable’ (Site A, Manager)
Findings: rational workarounds • ‘One of the obstetricians was telling me that they’re very reluctant to measure respiratory rates, when patients are being recovered from a Caesarean section, because if we have to do it we will then fail our CNST audit. There’s mixed messages coming out that actually this monitoring doesn’t have to be done until you see the woman breathing either very slowly or gasping’ (Site B, Anaesthetist)
Findings: rational workarounds and the normalisation of deviance • High activity levels legitimised non compliance with MEOWS charts. Non conformity became part of ‘the way things end up around here’ • Socially sanctioned by senior staff • ‘by giving them a MEOWS chart on the postnatal ward for 25 women, we’re setting them up to fail (Site A, Obstetrician) • ‘It would be much easier just to say, ‘Come on, you lot, all toe the line [with the MEOWS charts], you do it this way or else.’ But then, if you lose half your staff by doing it it’s pretty pointless, isn’t it’ (Site A, Manager)
Conclusions • Value of this work in understanding • Intended and unintended consequences of the tool • Naturalisation process (‘active standardisation work’, ‘work arounds’ • Normative standards reflected adaptability of the two organisations and consequences of ‘dark side’ of rule breaking/adherence
Questions • How do we best engage with clinicians and managers in feeding back results pertaining to both the ‘bright’ and ‘dark’ side of organisational work? • How do we facilitate changes at structural / cultural level rather than at team / task level? • What are the future research priorities?
Acknowledgements • Thank you: Staff and service user participants • Disclaimer: this presentation presents independent research commissioned by the National Institute for Health Research (NIHR). The views expressed in slides are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. • Contact: nicola.mackintosh@kcl.ac.uk http://www.kingspssq.org.uk/
Publications • Mackintosh, N. & Sandall, J. Overcoming gendered and professional hierarchies in order to facilitate escalation of care in emergency situations: The role of standardised communication tools: Social Science and Medicine. 71 (9):1683-6 • Mackintosh, N. & Sandall, J.Intelligent Assessment Tools in Heathcare: technological fix or the potential for unintended consequences? Accepted for CARR Publication Risk & Regulation, August 2010 • Mackintosh, N. & Sandall, J. (2008). Working Paper, ‘The management of failure to rescue’ http://www.kingspssq.org.uk/programmes/innovations/failure-to-rescue-problems-and-solutions/