Download
1 / 34
340 likes | 355 Views
This comprehensive guide by Dr. S. Parthasarathy covers the physiological changes, triggers, respiratory and muscle effects, blood-related issues, urological and gastrointestinal complications, psychological aspects, intrathecal baclofen pumps, pre-operative assessment, drug considerations, DVT risks, and anesthetic options for patients with chronic spinal cord injuries. The text includes insights on autonomic dysreflexia, spasticity management, and perioperative care strategies.

E N D
Perioperative management for patients with a chronicspinal cord injury Dr. S. Parthasarathy MD., DA., DNB, Dip. Diab., DCA, Dip. Software statistics- PhD ( physiology) , IDRA, FICA
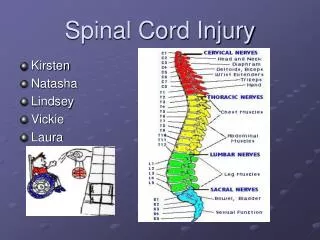
Spinal cord injury • First phase – one hour – sympathetic discharge and hypertension • Acute phase – shock – first eight weeks • Flaccid paralysis – areflexia • Hypotension , bradycardia • Myocardial dysfunction • Chronic phase – autonomic hyperreflexia
PHYSIOLOGICAL CHANGES IN CHRONIC SPINAL CORD INJURED PATIENTS
Autonomic dysreflexia (AD) • Level of injury T 6 or above • acute elevation of arterial blood pressure (BP) and bradycardia (slow heart rate), although tachycardia (rapid heart rate) also may occur. • Objectively, an increase in systolic BP greater than 20–30 mmHg is considered a dysreflexic episode • alterations in connections within the distal spinal cord lead to the abnormal sympathetic responses
Consequences • increase in pressure may cause • intracranial or retinal haemorrhage, • seizures, • myocardial ischaemia, • pulmonary edema and death. It may start any time between 3 weeks and 12 years of injury Vasodilation above – nasal congestion Mild facial edema !
Triggers – non surgical • Bladder distension • Colonic stimulus • Anal fissure • Uterine interventions • Misoprostone • Ingrowing toe nail • Pressure sore manipulation Sacral triggers ??
Clonidine for spastic ADR Intravesical capsaicin for bladder
Respiratory changes • Shallow respiration • Thoracic musculature weakness • Weak cough • Accessory muscles • Increased secretions • Leads on to atelectasis
Muscle • An increase in acetylcholine receptors on muscle membrane follows spinal injury. • Hyperkalaemia and cardiac arrest is a risk. • Increased muscle tone occurs in the reflex phase and a violent spasm may be caused by minor proprioceptive or cutaneous stimuli
Blood • Blood volume decreased • Postural hypotension ( IPPV ? ) • A normochromic, normocyticanaemia is common. • Hypoalbuminaemia may be present. • Risk of deep vein thrombosis in the initial stages of injury (up to 30%) • prophylaxis may include warfarin or unfractionated heparin for several weeks.
Others • Significant osteoporosis occurs in cord injured patients and predisposes them to fractures • A high spinal cord injury impairs the ability to shiver, vasodilate and sweat. • Prone for pressure sores and the inherent risks of the sores
Urology and GI • Urinary tract infection, proteinuria, reflux and calculi occur commonly. • Renal failure may rarely supervene. • An acute gastroparesis and ileus may occur after acute spinal cord injury. • Chronic spinal cord injured patients may have delayed gastric emptying.
Psychological complications of post SCI include depression, suicide, and drug addiction. • Chronic pain can complicate 60 % of cases • Renal and liver impairment can complicate certain cases
All changes • Pertain to T6 • If its C5 , changes may vary • 90 % of respiration – accessory muscles ?
Intrathecalbaclofen pumps • Baclofen pumps are used in patients which severe spasticity requiring large doses of anti-spasmodic medications precipitating unwanted side-effects. • The operation includes insertion of a lumbar or low thoracic catheter, tunnelled to the connecting pump that is inserted in the lower abdominal wall
PRE-OPERATIVE ASSESSMENT • Nature , Timing of neurological injury • Sensory and motor level. • Vagally mediated reflexes intact? – antispasmodics • The occurrence of autonomic dysreflexia will be revealed by questions about sweating, flushing, headache or directly about elevated blood pressure. • PFT and ABG SOS • I.V. access is often difficult because of atrophic, hyperaesthetic skin with reduced cutaneous blood flow.
Pre op drugs • Baclofen , tizanidine – can omit one dose • Diazepam, clonazepam – as adjuncts • Marijuana for spasticity • Oxybutinin is a frequently used anticholinergic drug. It is an antisialogogue and may enhance the sedative effects of general anesthetic agents.
DVT • Initial six weeks after injury – DVT is 85 % • Chronic – very less – no need for prophylaxis • Muscle spasticity and venous collapse attributed • But perioperative heparin advocated
ANAESTHETIC OPTIONS • Local • Regional • General • Can we do without anesthestist ?? NO 500 ml of Ringer – must
Spinal - YES • Spinal anesthesia is safe in patients with CSCI and is an effective way of abolishing ADR and spasms. (1.5 - 2 ml is enough for most procedures) • Spinal anesthesia is becoming a widely accepted technique in patients with pre-existing spinal cord pathology.. • Difficult to put ?? • Difficult to assess – babinski ? Flaccidty ?
Epidural • Epidural anesthesia has been demonstrated to be effective in reducing ADR in labouring women; • it is less reliable for general and urological surgical procedures. • Prolonged procedures and post op ADR prophylaxis – can be used
Nerve blocks • Upper limb surgery - brachial plexus block, • done under ultrasound guidance • nerve stimulators unreliable in the presence of cervical injuries. • Beware of phrenic injury • Go for axillary if acceptable !
Premed with ? Nifedipine • Lower doses of general anesthetics • Muscle mass is less ! VRG !! • volume of distribution ?? • Vasopressors use ? Prophylaxis ??
Scoline – 6 months old ? • Denervated muscle results in an increase of extrajunctional acetylcholine receptors, spreading from motor end-plate of affected muscle fibres to cover the whole muscle membrane • Beware of scoline
Airway • Positioning and difficult airway • RSI if ? • Laryngeal mask airway – OK • Aspiration risk is theoretical • Tracheostomy – change to cuffed tube ?
Fluid warmers are OK • No warm mattresses • Cant react fast to hypothermia
Recovery • Muscle function • Temperature • Sores and cautery pads • Respiration and oxygen
CSCI and pregnancy • Further reduction in respiratory reserve • Reduction in FRC • Prone for atelectasis and respiratory failure • Prone for urinary infections • DVT • Anemia Worsens ??
Level below T 10 – pain perceived • But ADR – onset of labour ?? • Epidural prior to onset of labour • Continue for 48 hours to abolish ADR
Summary • CSCI -Surgeries • Changes • ADR • Spinal • Epidural or GA • Post op • Labour