Download
1 / 1
40 likes | 324 Views
Design, Implementation and Evaluation of a Clinical Nurse Leader Model of Inpatient Medical –Surgical Nursing Care Grace Sotomayor, MSN, RN (DNP Student) Kay Sackett , PhD, RN ( Faculty Advisor) Dennis Taylor, DNP, RN ( Clinical Advisor)

E N D
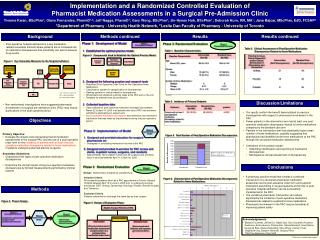
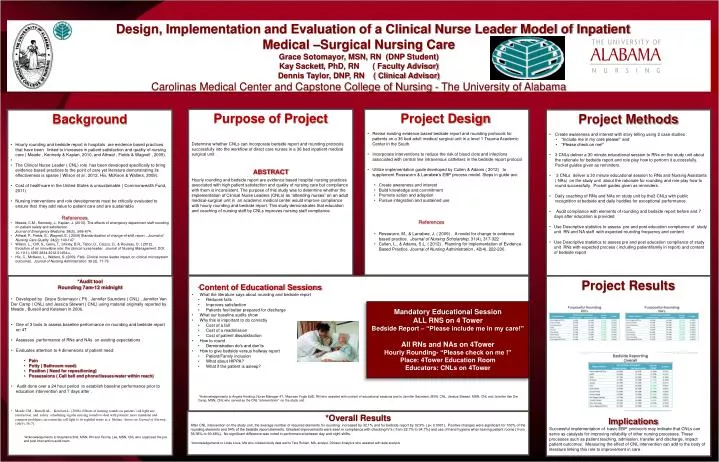
Design, Implementation and Evaluation of a Clinical Nurse Leader Model of Inpatient Medical –Surgical Nursing Care Grace Sotomayor, MSN, RN (DNP Student) Kay Sackett, PhD, RN ( Faculty Advisor) Dennis Taylor, DNP, RN ( Clinical Advisor) Carolinas Medical Center and Capstone College of Nursing - The University of Alabama • Project Design • Revise existing evidence based bedside report and rounding protocols for patients on a 36 bed adult medical surgical unit in a level 1 Trauma Academic Center in the South. • Incorporate interventions to reduce the risk of blood clots and infections associated with central line intravenous catheters in the bedside report protocol • Utilize implementation guide developed by Cullen & Adams ( 2012) to supplement Rosswurm & Larrabee’s EBP process model. Steps in guide are: • Create awareness and interest • Build knowledge and commitment • Promote action and adoption • Pursue integration and sustained use • References • Rosswurm, M., & Larrabee, J. ( 2009) . A model for change to evidence based practice. Journal of Nursing Scholarship, 31(4), 317-322 • Cullen, L., & Adams, S.L. ( 2012) . Planning for implementation of Evidence- Based Practice. Journal of Nursing Administration , 42(4), 222-230. • Purpose of Project • Determine whether CNLs can incorporate bedside report and rounding protocols successfully into the workflow of direct care nurses in a 36 bed inpatient medical surgical unit . • ABSTRACT • Hourly rounding and bedside report are evidence based hospital nursing practices associated with high patient satisfaction and quality of nursing care but compliance with them is inconsistent. The purpose of this study was to determine whether the implementation of Clinical Nurse Leaders (CNLs) as “attending nurses” on an adult medical-surgical unit in an academic medical center would improve compliance with hourly rounding and bedside report. This study demonstrates that education and coaching of nursing staff by CNLs improves nursing staff compliance. • Background • Hourly rounding and bedside report in hospitals are evidence based practices that have been linked to increases in patient satisfaction and quality of nursing care( Meade , Kennedy & Kaplan, 2010, and Athwal , Fields & Wagnell , 2009). • The Clinical Nurse Leader ( CNL) role has been developed specifically to bring evidence based practices to the point of care yet literature demonstrating its effectiveness is sparse ( Wilson et al , 2012, Hix, McKeon & Walters, 2009). • Cost of healthcare in the United States is unsustainable ( Commonwealth Fund, 2011) • Nursing interventions and role developments must be critically evaluated to ensure that they add value to patient care and are sustainable • References • Meade, C.M., Kennedy, J., Kaplan, J. (2010). The effects of emergency department staff rounding on patient safety and satisfaction. • Journal of Emergency Medicine, 38(5), :666-674. • Athwal, P., Fields, E., Wagnell, E. ( 2009) Standardization of change-of-shift report.. Journal of Nursing Care Quality 24(2): 143-147 • Wilson. L., Orff, S., Gerry, T., Shirley, B.R., Tabor, D., Caizzo, D., & Rouleau, D. ( 2012). Evolution of an innovative role: the clinical nurse leader. Journal of Nursing Management, DOI: 10.1111/j.1365-2834.2012.01454.x. • Hix, C., McKeon, L., Walters, S. (2009, Feb). Clinical nurse leader impact on clinical microsystem outcomes. Journal of Nursing Administration. 39 (2), 71-76 • Project Methods • Create awareness and interest with story telling using 2 case studies : • “Include me in my care please!” and • “Please check on me!” • 3 CNLs deliver a 30 minute educational session to RNs on the study unit about the rationale for bedside report and role play how to perform it successfully. Pocket guides given as reminders. • 3 CNLs deliver a 30 minute educational session to RNs and Nursing Assistants ( NAs) on the study unit about the rationale for rounding and role play how to round successfully. Pocket guides given as reminders. • Daily coaching of RNs and NAs on study unit by the3 CNLs with public recognition at bedside and daily huddles for exceptional performance. • Audit compliance with elements of rounding and bedside report before and 7 days after education is provided • Use Descriptive statistics to assess pre and post education compliance of study unit RN and NA staff with expected rounding frequency and content • Use Descriptive statistics to assess pre and post education compliance of study unit RNs with expected process ( including patient/family in report) and content of bedside report • *Audit tool • Rounding 7am-12 midnight • Developed by Grace Sotomayor ( PI) , Jennifer Saunders ( CNL) , Jennifer Van Der Camp ( CNL) and Jessica Stewart ( CNL) using material originally reported by Meade , Bursell and Ketelsen in 2006. • One of 3 tools to assess baseline performance on rounding and bedside report on 4T • Assesses performance of RNs and NAs on existing expectations . • Evaluates attention to 4 dimensions of patient need: • Pain • Potty ( Bathroom need) • Position ( Need for repositioning) • Possessions ( Call bell and phone/tissues/water within reach) • Audit done over a 24 hour period to establish baseline performance prior to education intervention and 7 days after . • Meade CM ., Bursell AL ., Ketelsen L. (2006). Effects of nursing rounds on patients' call light use, satisfaction, and safety: scheduling regular nursing rounds to deal with patients' more mundane and common problems can return the call light to its rightful status as a lifeline. American Journal of Nursing, 106(9), 58-71. • . • *Acknowledgements to Stephanie Britt, MSN, RN and Tammy Lee, MSN, CNL who organized the pre and post intervention audit team. • *Content of Educational Sessions • What the literature says about rounding and bedside report • Reduces falls • Improves satisfaction • Patients feel better prepared for discharge • What our baseline audits show • Why this is important to do correctly • Cost of a fall • Cost of a readmission • Cost of patient dissatisfaction • How to round • Demonstration do’s and don’ts • How to give bedside versus hallway report • Patient/Family inclusion • What about HIPPA? • What if the patient is asleep? • *Acknowledgements to Angela Hosking, Nurse Manager 4T, Maureen FogleEdD, RN who assisted with content of educational sessions and to Jennifer Saunders, MSN, CNL, Jessica Stewart, MSN, CNL and Jennifer Van Der Camp, MSN, CNL who served as the CNL “interventions” on the study unit. • Project Results • Implications • Successful implementation of basic EBP protocols may indicate that CNLs can serve as catalysts for improving reliability of other nursing processes. These processes such as patient teaching, admission, transfer and discharge, impact patient outcomes. Measuring the effect of CNL intervention can add to the body of literature linking this role to improvement in care . Mandatory Educational Session ALL RNS on 4 Tower Bedside Report – “Please include me in my care!” All RNs and NAs on 4Tower Hourly Rounding- “Please check on me !” Place: 4Tower Education Room Educators: CNLs on 4Tower *Overall Results After CNL intervention on the study unit, the averagenumber of required elements for rounding increased by 32.1% and for bedside report by 32.9% ( p< 0.0001). Positive changes were significant for 100% of the rounding elements and 54% of the bedside report elements. Greatest improvements were seen in compliance with checking IV’s ( from 22.7% to 94.7%) and use of hand hygiene when leaving patient rooms ( from 36.36% to 90.48%). No significant difference was noted in performance between day and night shifts. *Acknowledgements to Linda Louis, MA who collated study data and to Tara Ruhlen, MA, analyst, Dickson Analytics who assisted with data analysis.