Download
1 / 18
200 likes | 481 Views
Active Insulin Infusion Control of the Blood Glucose Derivative. J G Chase, Z-H Lam, J-Y Lee and K-S Hwang University of Canterbury Dept of Mechanical Engineering Christchurch New Zealand ICARCV 2002, Singapore. Silicon + Biology?.

E N D
Active Insulin Infusion Control of the Blood Glucose Derivative J G Chase, Z-H Lam, J-Y Lee and K-S Hwang University of Canterbury Dept of Mechanical Engineering Christchurch New Zealand ICARCV 2002, Singapore
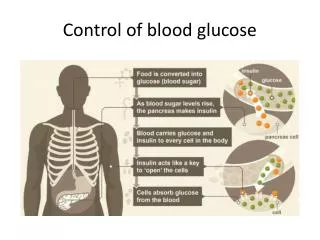
Silicon + Biology? • Many biological and/or medical processes are effectively feedback control systems or can have their function replaced by feedback systems • New technology creating new possibilities: • “BioMEMS” such as “wet sensors” and “gene chips”, are opening the path to real time physiological monitoring/sensing and actuation. • Wireless technology (LAN and PAN) for communication between active elements and/or monitoring technology (increased information flow). • Advanced embedded computers (DSP’s) and real time operating systems (RTOS’s) can now handle extensive calculations and operations required. Converging technologies enables the ability to monitor, control and/or replace dysfunctional physiological behaviour(s). • Can the increased information from real-time sensing coupled with feedback control outperform the foreknowledge and intuition of an experienced diabetic??
3 Elements of Control Systems • Sensing • Real-time sensing from GlucoWatch or similar technology at BW = 20 minutes or greater • Computation • Modern embedded DSP’s are far more than adequate • Actuation • Insulin pump • All are existing and near-term technologies • Must account for limitations of existing tech and determine the limits where practicality and feasibility occur together.
Type I Blood Glucose Level over Basal IGT, Type II Normal Time Ideal curve is flat! 2-3 hours Back to Fasting Level Diabetes • Current Treatment = Manual Monitoring + Injection = Error Prone Diabetes is reaching epidemic proportions, treatment is dependent on unreliable individuals and has not changed significantly in 30+ years • GOALS: • Automate the “5:95” (1 day every 3 weeks is “bad”) • Account for variations in patient response, insulin employed, sensor bandwidth and actuator dynamics/limits.
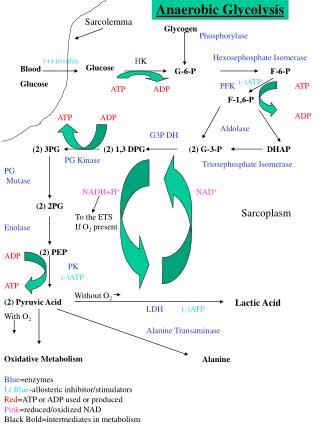
System Model • System model is constructed in MATLAB/Simulink. • Three parts: one part for each equation in model and controller. • Controller: input - G and dG/dt (GlucoWatch) and output u(t) (Insulin Pump)
Controllers • Relative proportional controller (RPC). • PD controller – controls slopes of incresing/decreasing blood sugar level rather than actual glucose concentration Two controllers, one proportional based and the other derivative weighted where Kp << Kd create two different approaches to control Shapecontrol orMagnitudecontrol
Peak glucose level – Proportional control is most active here Glucose level is still positive. The slope is the highest here – Derivative control most active here Slope (derivative) is negative Why “Heavy Derivative” Control? • Derivative control - negative slope prevents further insulin injection when the • glucose level is dropping and faster reaction to positive surge.
Control of Glucose Tolerance Test RPC – BW = 20 min • As sampling rate increases, the more effective the controllers become. • Optimal control: G is very nearly flat as desired
RPC – sensor BW = 20 min Insulin Infusion Rates for GTT • PD controller minics what a diabetic would usally do, a routine optimised over 70 years of clinical treatment. • Insulin rates are sharper and nearer injections as sensor BW drops.
A More Difficult Test • 1000 calories in 4 hours over five “meal” inputs of glucose which is rapidly absorbed • Inputs vary in magnitude from 50 – 400 calories • Inputs occur in two groups of rapid succession at t = 0, 10, 30 minutes and at t = 210 and 300 minutes • The last meal is 40 calories from 980 – 1020 calories so the full absorption of about 1000 calories occurs by 4 hours quite easily. • Controller has no knowledge of glucose input except in optimal case • Input knowledge is not currently practicable in any way for this system in general The goal is to “hammer” the system and see if it breaks!
Control of Glucose Inputs • Glucose excursions shrink with sensor BW • Optimal control very nearly flat as desired • Simple PD control emphasizes derivative over proportional inputs by 100
Normal and Diabetic Glucose Response • Response of a normal subject to Glucose Input (orange) • PD controller developed is slightly better than normal subject by • 7-25% on peak value and 1+ hour in return to basal glucose level
Insulin rates are sharper and nearer injections expected as sensor BW drops • Lower insulin rates less effective control as might be expected. Insulin Infusion Rates for Glucose Inputs
Relative Proportional Control Comparison u(t)=Uo(1+Kp(G/Gb)) Danger @ -1.5 Death @ -3 • Relative proportional control more robust to Hypoglycemic behaviour
PD Controller against Sensor Lag (RPC) • GlucoWatch™ (glucose sensor) has 20 minute sensor lag • PD Controller ROBUST against 20 minute sensor lag • The peak is slightly increased, but less hypoglycemic response
PD Controller against Sensor Failure • Sampling bandwidth = 20 minutes • PD controller ROBUST against 20 minute failure • Hypoglycemia induced for 60 minute failure
Summary & Conclusions • Bergman equations found to very suitable for control systems approach • Feasibility of automated insulin infusion is shown in simulation • Basic tradeoffs between sensor BW and control efficacy delineated • Derivative control or “control of slopes” seen to be the most effective form of feedback so far versus proporational dominated or relative proportional. • Insulin inputs with derivative control trending towards matching those of “optimized” insulin injection regimes followed by diabetics.
Ongoing Future Work = First Known Trials • Kidney Failure • Dialysis Machine • 67 year old Female • High fluid levels • 3rd day in ICU • Hyper-insulinemic • and Hyper-glycemic GlucoCard error = 7%