Download
1 / 89
890 likes | 1.07k Views
IDEA 2004 for EHDI Professionals. 2012 EHDI Conference Sharon S. Ringwalt, Ph.D., CCC-SLP National Early Childhood Technical Assistance Center (NECTAC ), Mid-South Regional Resource Center (MSRRC ), and Temporary Assignment to CDC EHDI Team. What is IDEA?.

E N D
IDEA 2004 for EHDI Professionals 2012 EHDI Conference Sharon S. Ringwalt, Ph.D., CCC-SLP National Early Childhood Technical Assistance Center (NECTAC), Mid-South Regional Resource Center (MSRRC), and Temporary Assignment to CDC EHDI Team
What is IDEA? • Individuals with Disabilities Education Improvement Act (IDEA 2004) • Originally passed in 1975 as the Education for All Handicapped Children Act • Established framework for special education and early intervention services in this country • Reauthorization signed December 3, 2004
Historical Overview of IDEA • 1975 – Congress passed PL 94-142 (Education of All Handicapped Children Act) • 1986 - PL 99-457 • Section 619 (added preschool) • Part H (became Part C) • 1997 - IDEA reauthorized • 2004 – passed the Individuals with Disabilities Education Improvement Act 2004 • September 2011 – new Part C regulations issued
The Law of the Land • The Individuals with Disabilities Education Act (IDEA) provides a free, appropriate, public education for all children with disabilities, including speech, language, and hearing disorders. Part B funds cover children ages 3-21. Services are provided as outlined in the Individualized Education Program (IEP). Part C funds cover infants from birth through age two and services are provided as outlined in the Individualized Family Service Plan (IFSP). • Part B services are mandatory; Part C services are not.
IDEA 2004 • Signed into law December 3, 2004 • NEW NAME (i.e., includes IMPROVEMENT!) but same acronym • NPRM: Proposed Code of Federal Regulations for Part B (services for children 3-21) released June 10, 2005; newPart C regulations issued September 2011 • Statute Implementation: July 1, 2005; New Part C Regulations Implementation: July 1, 2012
IDEA 2004: Purpose • To ensure all children with disabilities have available to them a free appropriate public education • To ensure the rights of children with disabilities and their parents are protected • To assist education agencies to provide for the education of all children with disabilities • To assist States in the implementation of early intervention services for infants and toddlers with disabilities and their families • To ensure that educators and parents have the necessary tools to improve educational results for children with disabilities
IDEA 2004: Part C Purpose • To develop and implement a • statewide • comprehensive, • coordinated, • multidisciplinary • system of support and services • for infants and toddlers with disabilities • and their families
What are Some of the new IDEAs? • Early Intervening Services allow use of up to 15% of special education funds to be used for pre-referral activities • Allows for use of a Response to Intervention model in determining LD • Need to document what you are doing and how you are doing it!
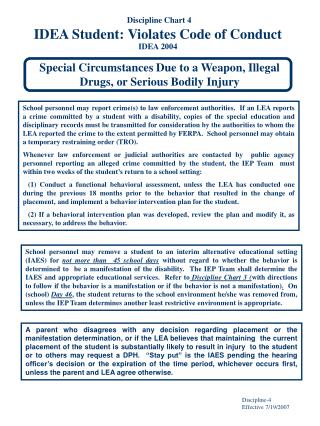
What are other NEW IDEAs? • Due Process changes for Part B • Parents must notify districts of their specific issues at the time that they file a written complaint • Two years statute of limitations instead of three • The party requesting the hearing shall not be allowed to raise issues at the hearing that were not raised in the due process complaint notice, unless the other party agrees
More on IDEA 2004 • Assistive Technology - not considered a surgically implanted medical device (i.e., cochlear implant, prosthesis) NOR is it considered a related service • Highly Qualified Teachers – SPED teachers must be NCLB HQ + SPED certified • Related Services includes nursing services
More on IDEA 2004 • Addresses specific concerns about ELLs • References Homeless • Includes definition of universal design • Mandates provision of instructional materials for students with print disabilities through the National Instructional Materials Access Center • Increases the benefits afforded private school students
Reauthorization of IDEA 2004 – Highlights 13 • Implications for Audiology • Policy direction provided on the need to provide information on “the full range of options to families of deaf and hard of hearing children” • Addition of “interpreting services” as an identified related service • Identification of “teachers of the deaf” as special educators
Reauthorization of IDEA 2004 – Highlights, continued • Implications for Audiology • States given flexibility to define personnel qualifications • Retention of Regional and State centers (schools) for children, when this is the least restrictive environment (LRE) • Establishment of both “cued language services” and “sign language [services]” as early intervention (EI) services
IFSP Process • From Referral to Service Delivery • See NECTAC handout (also http://www.nectac.org/~pdfs/topics/families/ifsp_process_chart.pdf) (currently being revised to incorporate changes in new Part C regs)
Child Find: Identification and Referral • Potential Referral Sources: • From EHDI Program • From Hospitals • From Physicians • From Families • From Child Care Providers • From Other Community Programs • Other?
Intake and Family Assessment • Varies from state-to-state • Service Coordinator – Interim or permanent • Includes finding out families needs, priorities, goals
Child Evaluation and Assessment • 3 potential steps: screening, evaluation, and assessment • Use assessment in program planning and for progress monitoring • Apply data collection/assessment to decision-making process • Eligibility varies widely from state-to-state, including eligibility of children with hearing loss
IFSP Development • Developed by a TEAM, not a single individual • Must include the family
Service Delivery and Transition • Services must be delivered in a child’s natural environment • Transition begins with the very first IFSP meeting • Transition includes specific requirements; some changes with new Part C regs
Requirements?What Requirements? • New Part C regs: http://www.gpo.gov/fdsys/pkg/FR-2011-09-28/pdf/2011-22783.pdf • What do the data tell us?
How would they each use data? OSEP • quality assurance • reporting to stakeholders • control costs • establish provider credentials • determine what services covered Private Insurance Medicaid • predict resource utilization • establish eligibility criteria • develop data driven payment mechanisms • assist employers w/decisions about benefit packages • distinguishing between educational and medical necessity • determine reimbursement rates • improve coding
National Focus: SPP/APR • SPP = State Performance Plan • 6 year plan, developed by each state in 2005; extended for 2 more years (until next reauthorization?!?) • APR = Annual Performance Report • Completed yearly by each state, submitted in February • Covers data from the previous FFY (Federal Fiscal Year) – e.g., the APR submitted February 2012 reported data from FFY 2010 (July 2010 through June 2011)
Compliance Indicators – Part C • C1 – Timely Service Delivery • C7 – Timeliness of IFSP • C8 – Early Childhood Transition (A, B, C) • C9 – Part C Monitoring System • C10 – Administrative Complaints • C11 – Due Process Hearings • C14 – Data Accuracy
Results (Performance) Indicators: Part C • C2 – Settings • C3 – Child Outcomes (A, B, C) • C4 – Family Outcomes • C5 – Child Find, Ages Birth to 1 • C6 – Child Find, Ages Birth to 3 • C12 – Resolution Agreements • C 13 – Mediations
What does “compliance” mean? • State’s target MUST be 100% • Affects State’s “Determination” • Meets requirements • Needs assistance • Needs intervention • Needs substantial intervention • State must report all non-compliance
What does “results” mean? • State sets its own targets, based upon stakeholder input • Has not affected State’s “Determination” – but may in future • State must report all non-compliance
States’ Focus • Accountability • Data – systems, quality, validity, reliability • Finance • MOE (maintenance of effort) • FAF (Federal Allocation Formula)/FMAP (Federal Medical Assistance Percentage) • Reimbursement – Insurance, Medicaid, Family Co-Pay, other sources • ARRA funds – must have been expended by 12/31/11 • Quality services • Evidence-based practices • Family and provider satisfaction
New Accountability Measures • In Fall 2011, OSEP began new 4-year cycle of continuous improvement and monitoring visits • 2-3 days focusing on “verification” • NEW for Fall 2011: 1-2 days focusing on “results” • After the first round of Results Visits, process being reviewed and refined • First-round states chose to focus on child find, child outcomes or family outcomes
Accountability • Providers whose agencies receive Part C funds are responsible for implementing all IDEA requirements. • Compliance Indicators • Results Indicators • Related Requirements
Maintenance of Effort • States must maintain their (fiscal) effort each year – the same or additional state dollars must be allocated to Part C each year • Implications: • States’ continued participation in Part C • Bifurcated system • Changes in eligibility • What might each of these mean for children with hearing loss; • with speech-language delays or disorders?
Legislative Mandate • Recent federal legislation requires that early intervention services and supports be provided to the maximum extent appropriate in natural environments, including the home and community settings in which children without disabilities participate (IDEA, 2004, SEC 632 G).
Legislative Mandate • According to IDEA 2004, services and supports should be provided in a setting other than a natural environment only when early intervention cannot be achieved satisfactorily in a natural environment (IDEA, 2004, SEC 632 G). • In those cases, written justification must be provided.
What does this mean for You? • What are the implications of this legislative mandates for those who deliver services to infants and toddlers who are deaf or hard of hearing? For the families of these children?
Determinations • OSEP makes states’ determinations • Announced in early June • States must make determinations of local programs, considering: • Performance on compliance indicators; • Whether data submitted by LEAs/EIS programs is valid, reliable, and timely; • Uncorrected noncompliance from other sources; and • Any audit findings.
Important Transitions Currently Occurring in Service Delivery • Focus on family-centered practices & principles • Emphasis placed by legislation and “recommended practices” on delivery of service in natural environments • Move from primary direct service delivery model to a range of service delivery options
What Are Natural Environments? • Families’ homes • Early care and education settings • Community settings (e.g., park, recreation facility, play groups) • Any place that families and IFSP team members indicate is a desired location for intervention
Benefits of Service Delivery in Natural Environments • Natural learning opportunities are important for promoting children’s development and functioning (Dunst, Bruder, Trivette, Hamby, Raab, & McClean, 2001). • Families report enhanced feelings of security and control over services being provided in their home and increased family support structure (Stowe & Turnbull, 2001).
Benefits of Natural Environments • The basic premise of intervention in natural environments is the involvement of the family and caregivers in the teaching and learning process with children as they communicate throughout the day (Bruder, 1998). • SLP has concrete opportunities to assess the child in daily activities as they occur and demonstrate how to embed intervention into these activities, increasing the accuracy and frequency of communication opportunities for the child and caregivers (Cripe & Venn, 1997).
Benefits of Service Delivery in Community Settings • Support and encouragement from others outside the family • Improvement in child self-esteem • Facilitation of social skills, adaptive skills, and positive behavior through peer modeling • Enhanced sense of belonging on the part of the family (Bruder, 2001;Stowe & Turnbull, 2001)
Goal of early intervention “…To enable young children to be active and successful participants during the early childhood years and in the future in a variety of settings – in their homes with their families, in child care, in preschool or school programs, and in the community.” (from Early Childhood Outcomes Center, http://www.fpg.unc.edu/~eco/pdfs/eco_outcomes_4-13-05.pdf)
CDC: Newborn Hearing Screening and Diagnosis • In 2009, the Centers for Disease Control and Prevention (CDC) data showed that over 97% of newborns in the United States were screened for hearing loss. • Of those who were screened, 1.6% did not pass the final or most recent hearing screening. • Of those babies not passing the hearing screening, 67.9% were diagnosed as either having or not having a hearing loss before 3 months of age. • There was an increase in the number of infants screened for hearing loss from 1999 (46.5%) to 2007 (97.0%).
Part C Services for Babies with Hearing Loss • In 2009, 88.0% of the babies with diagnosed hearing loss were referred to Part C Early Intervention Services. • Among the 88% of those referred, 91% were eligible for Part C services • The remaining 9% referred either were not eligible for services or their eligibility status was unknown.
Issues between EHDI and Part C • Loss to follow-up/loss to documentation • Eligibility criteria • Child and family privacy • Data sharing
In 2005 and 2006, more than 90% of infants were screened for hearing loss. Of these infants, 2% in both years did not pass their final screening. Out of those not passing the final screening, approximately two-thirds were not documented as having a diagnostic finding. In both years, the reason reported for the majority of infants was loss to follow-up/loss to documentation (LFU/LTD). Although the majority of infants with permanent hearing loss were receiving intervention, more than 30% were classified as LFU/LTD and could not be documented as receiving intervention services.(Gaffney, Green, & Gaffney, Publication Information: Public Health Reports / March–April 2010 / Volume 125 (pages 199 – 207) (www.publichealthreports.org/archives/issuecontents.cfm?Volume=125&Issue=2)