Download
1 / 68
690 likes | 833 Views
advanced hodgkin lymphoma. robert r johnson november 18, 2010. epidemiology. estimated 8220 new cases and 1350 deaths in U.S. this year incidence of 3 per 100,000 slight male predominance 1.1 to 1 median age at diagnosis is 26 bimodal peaks in incidence early: 15-30 late: > 55.

E N D
advanced hodgkin lymphoma robert r johnson november 18, 2010
epidemiology • estimated 8220 new cases and 1350 deaths in U.S. this year • incidence of 3 per 100,000 • slight male predominance • 1.1 to 1 • median age at diagnosis is 26 • bimodal peaks in incidence • early: 15-30 • late: > 55
epidemiology • proposed relationship between hodgkin lymphoma and epstein-Barr virus • ebv detected in tissue biopsies • higher levels of antibodies to ebv capsid in patients with hodgkin lymphoma • increased risk among individuals with history of infectious mononucleosis • smoking?
natural history • hallmark is painless lymphadenopathy • 80% present with cervical lymph node involvement • mediastinal mass on routine radiograph • 50% have mediastinal disease at time of diagnosis • 90% present with contiguous sites of involvement
natural history • may develop visceral involvement • direct extension from adjacent lymph nodes • hematogenous spread • also may involve bone and bone marrow • spleen considered contiguous site from para-aortic nodes • nearly always precedes visceral or bone marrow disease • gut-associated lymphoid tissues rarely involved • waldeyer’s ring, peyer’s patches
natural history • one third patients present with systemic symptoms • typically “b” symptoms • fever, drenching night sweats, weight loss > 10% over previous 6 months • prognostic significance and part of staging • fevers and weight loss have worse prognosis
work-up • history and physical exam • b symptoms, palpable lymphadenopathy • laboratory • cbc, renal panel, lfts, esr, pregnancy test • imaging • ct, pet/ct, echo (preparation for doxorubicin) • tissue biopsy • excisional lymph node biopsy preferred • bone marrow biopsy • indicated in presence of b symptoms or subdiaphragmatic disease
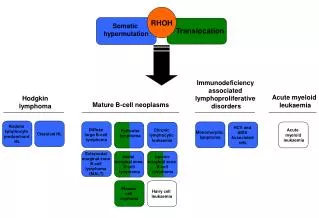
pathology • reed-sternberg cell is pathognomonic • dorothy reed mendenhall and carlsternberg • derived from b lymphocytes • multi-nucleated (owl’s eye) • eosinophilic nucleoli • stain positive for • cd15 and cd30 • stain negative for • cd20 and cd45
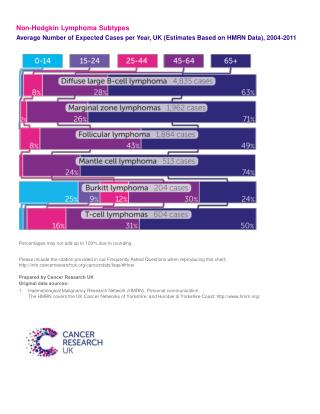
pathology • four classical histologic subtypes • nodular sclerosis Hodgkin lymphoma • 60-75% cases in u.s. • variable proportion of r-s cells • mixed-cellularity hodgkin lymphoma • 5-15% cases in u.s. • equal numbers of normal lymphocytes, r-s cells • lymphocyte-rich classical hodgkin lymphoma • 5% cases in u.s. • mostly normal lymphocytes, few R-S cells • lymphocyte depletion hodgkin lymphoma • < 5% cases in u.s. • abundant r-s cells
history and classification • advanced hodgkin lymphoma • stages ii (bulky or b symptoms), iii, iv • ~ 40% patients at presentation • traditionally a fatal disease • incurable with radiation alone • chemotherapy initially allowed for disease regression but rarely cure
international prognostic index • developed from 5000 patients with advanced hodgkin lymphoma • most treated with doxorubicin-based chemotherapy hasenclever et al. n engl j med.1998;339:1506-1514.
ipi hasenclever et al. n engl j med.1998;339:1506-1514
management • chemotherapy • mopp • abvd • stanford v • beacopp • radiotherapy • toxicity
mopp • mechlorethamine • nitrogen mustard • sometimes substituted for cyclophosphamide • Copp • vincristine (oncovin) • procarbazine • prednisone
mopp • discovered in 1960s at nci • allowed for cure of > 50% patients
first experience with mopp • 43 patients consecutive patients with advanced (stages iii and iv) hodgkin lymphoma • 1964-1967 • treated at nci • no “significant prior therapy” allowed • 1 course of chemotherapy • 1-2 courses of localized radiotherapy devita et al. ann intern med. 1973;73:881-895.
nci • work-up included h & p, labs, radiographs, lymphoscintigraphy, bone marrow biopsy • ct scanners not available until 1970s • patients treated with 6 cycles of mopp • 12 received cyclophosphamide instead of nitrogen mustard devita et al. ann intern med. 1973;73:881-895.
nci • 81% complete response rate • of responders • 4-year • disease free survival 47% • overall survival 77% • median survival 42 months • all patients • 4-year overall survival 63% devita et al. ann intern med. 1973;73:881-895.
nci • acute and chronic toxicity “generally tolerable” • mostly hematologic, neurologic, alopecia • no comment on reproductive function or second malignant neoplasms • results don’t sound that good, but… devita et al. ann intern med. 1973;73:881-895
nci • much better than historical data with single agent alkylators or vinca alkaloids • 10-25% cr rate • ~ 50% 2-year overall survival
toxicity of mopp • acute myelosuppression • gonads • especially in men • complete azospermia in ~ 80-100% • second malignant neoplasms • hematologic cancers from nitrogen mustard
abvd • developed in 1970s by giovanni bonadonna • given in 28 day cycles • 2-4 cycles for early stage hl • 6-8 cycles for advanced stage hl
abvd • less gonadotoxic and leukemogenic than mopp • more cardiac and pulmonary toxicity • doxorubicin and bleomycin viviani et al. eur j cancer clin oncol. 1985;21:601-605.
abvd vs mopp • 361 patients with stage iii and iv disease • 3 chemotherapy arms • 6-8 cycles of mopp • 6-8 cycles of abvd • 12 cycles of mopp alternating with abvd • 5-year • ffs 50% vs 61% vs 65% • os 66% vs 73% vs 75% (ns) canellos et al. n engl j med.1992;327:1478-1484.
abvd vs mopp • equal numbers of second malignant neoplasms • solid tumors and leukemias canellos et al. n engl j med.1992;327:1478-1484.
milan • 232 patients with stage iib, iiia, iiib disease • 6 cycles of abvd or mopp • radiotherapy between cycles 3 and 4 • 7-year • ffp 80.8% vs 62.8% • os 77.4% vs 67.9% • both significant santoro et al. j clin oncol.1987;1:27-37.
milan • toxicity profile better with abvd • irreversible gonadal dysfunction and acute leukemia only seen with mopp • no significant differences in cardiac or pulmonary toxicity santoro et al. j clin oncol.1987;1:27-37.
alternative chemotherapy regimens • stanford v • beacopp
stanford v • developed at stanford university in 1988 • lower doses of nitrogen mustard, bleomycin, doxorubicin (relative to mopp and abvd) • less hematologic, pulmonary, cardiac toxicity • 12 week schedule • intended to be given with 36 gyifrt • > 5 cm before chemo, macroscopic splenic disease
ecog 1492 ffp • phase ii study of 47 patients with bulky mediastinal stage i/ii or stage iii/iv hl • 12 weeks of stanford v followed by 36 gyifrt • median f/u 4.8 years • 5-yr • ffp 85% • os 96% os horning et al. j clin oncol.2000;18:972-980.
stanford • 142 patients with bulky mediastinal stage i/ii or stage iii/iv hl • 12 weeks of stanford v followed by 36 gy ifrt • median f/u 5.2 years • 5-yr • ffp 89% • os 96% horning et al. j clin oncol.2002;20:630-637.
stanford *statistically significant
toxicity with stanford v • predominantly hematologic • no acute grade 5 toxicity • 2 smns in patients treated on ecog 1492 and at stanford • 1 aml, 1 nsclc • 85% women in stanford group had regular menses • 43 children conceived after treatment horning et al. j clin oncol.2000;18:972-980., horning et al. j clin oncol.2002;20:630-637.
isrctn 64141244 • 6-8 cycles of abvd • 36 gyifrt if no cr after chemotherapy • 12 weeks of stanford v followed by 36 gy to bulky nodes or macroscopic splenic disease hoskin et al. j clin oncol.2009;27:5390-5396.
isrctn 64141244 • median f/u 4.3 years • 5-year • pfs • 76% for abvd • 74% for stanford v • os • 90% for abvd • 92% for stanford v • more non-pulmonary toxicity with stanford v • 19% vs 8% grade 3-4 • mostly hematologic hoskin et al. j clin oncol.2009;27:5390-5396.
isrctn 64141244 • similar efficacy of stanford v and abvd • stanford v arm did not perform as well as prior prospective studies • only 73% patients on isrctn study received rt • 91% on prior studies
beacopp • developed by ghsg for advanced hl • usually given in 21 day cycles • 2 variants: basic and escalated
ghsg hd9 engert et al. j clin oncol.2009;27:4548-4554.
ghsg hd9 • median f/u 10 years • 10-year fftf • 64% for copp/abvd • 70% for beacoppbase • 82% for beacoppesc • 10-year os • 75% for copp/abvd • 80% for beacoppbase • 86% for beacoppesc • beacoppesc significantly better for fftf and os engert et al. j clin oncol.2009;27:4548-4554
ghsg hd9 engert et al. j clin oncol.2009;27:4548-4554
ghsg hd9 • significantly more • hematologic toxicity with beacoppesc • aml/mds with beacoppesc • 3.2% vs 2.2% vs 0.4% • no difference in 10-year smn • 5.3% copp/abvd • 7.9% beacoppbase • 6.5% beacoppesc engert et al. j clin oncol.2009;27:4548-4554
alternative chemotherapy • stanford v • effective alternative to abvd • relatively safe • less pulmonary, cardiac, and gonadal toxicity than abvd or mopp • must be given with ifrt • beacopp • best survival outcomes • beacoppesc • significantly more toxicity • international prognostic index applies
involved-field radiotherapy • indicated for patients with early stage hl • role not as clear for advanced hl • mopp, abvd, beacopp • indicated for patients treated with stanford v
ifrt • 161 patients who achieved cr with mopp • 52 patients relapsed young et al. cancer.1978;42:1001-1007.
eortc 20884 24 gy to initially involved nodal areas, 16-24 gy to initially involved extra-nodal sites aleman et al. n engl j med.2003;348:2396-2406
eortc 20884 • median f/u 79 months • 5-year • efs 84% vs 79% (ns) • os 91% vs 85% (p = 0.07) • both favoring no rt • toxicity • 16% grade 3-4 hematologic toxicity during rt • no acute grade 5 • smn • 8% with rt • 4% without rt aleman et al. n engl j med.2003;348:2396-2406.
eortc 20884 30 gy to initially involved nodal areas (4-10 gy boost as indicated), 18-24 gy to initially involved extra-nodal sites aleman et al. int j radiat oncol biol phys.2007;67:19-30.
eortc 20884 • 8-year efs • 76% for pr-rt, 73% for cr-rt, 77% for cr-no rt • 8-year os • 84%, 78%, 85% aleman et al. int j radiat oncol biol phys.2007;67:19-30.