Download
1 / 4
40 likes | 294 Views
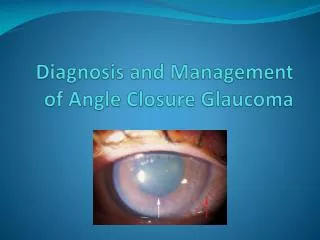
Anterior Segment Reconstruction in the Treatment of Chronic Angle Closure Glaucoma. Ivanov D.I. Katayeva Z.V. Bardasov D.B. IRTC “Eye Microsurgery ” Ekaterinburg Center. Financial interest: No.

E N D
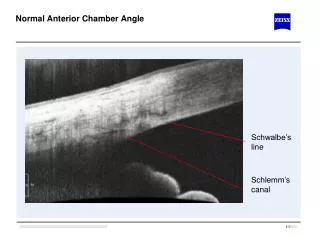
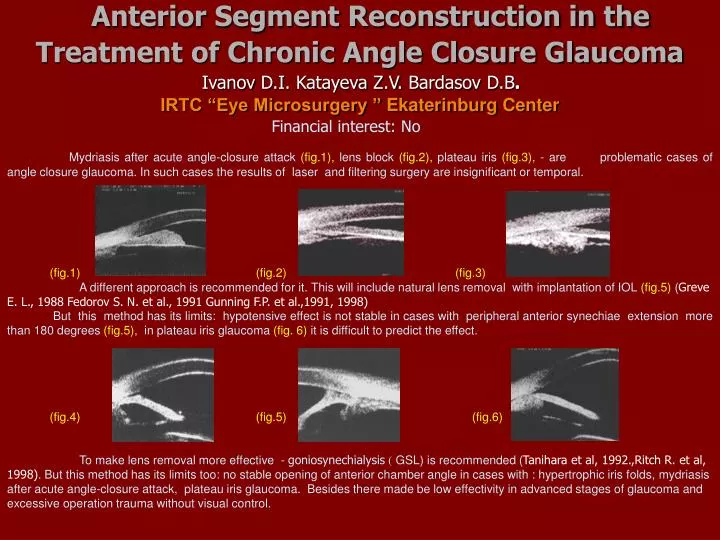
Anterior Segment Reconstruction in the Treatment of Chronic Angle Closure Glaucoma Ivanov D.I.Katayeva Z.V. Bardasov D.B. IRTC “Eye Microsurgery ” Ekaterinburg Center Financial interest: No Mydriasis after acute angle-closure attack (fig.1), lens block (fig.2), plateau iris (fig.3), - are problematic cases of angle closure glaucoma. In such cases the results of laser and filtering surgery are insignificant or temporal. (fig.1) (fig.2) (fig.3) A different approach is recommended for it. This will include natural lens removal with implantation of IOL (fig.5) (Greve E. L., 1988 Fedorov S. N. et al., 1991 Gunning F.P. et al.,1991, 1998) But this method has its limits:hypotensive effect is not stable in cases with peripheral anterior synechiae extension more than 180 degrees (fig.5), in plateau iris glaucoma (fig. 6) it is difficult to predict the effect. (fig.4) (fig.5) (fig.6) To make lens removal more effective - goniosynechialysis ( GSL) is recommended (Tanihara et al, 1992.,Ritch R. et al, 1998). But this method has its limits too: no stable opening of anterior chamber angle in cases with : hypertrophic iris folds,mydriasis after acute angle-closure attack, plateau iris glaucoma. Besides there made be low effectivity in advanced stages of glaucoma and excessive operation trauma without visual control.
Purpose : tointroduce thetechnologyincreasing effectivityofanglereconstructionwithcrystallinelensremovaland IOL implantation(fig.1,2)inproblematic cases ofangle-closureglaucoma - intraoperative visual gonioscopic control after manipulations in the anterior chamber angle(fig.3,6,8) - moving of iris folds from iris root towards central zone (fig.5) - irisfixation with sutures(fig.7) Thetechnologyincludes: Basis of the method The lens is removed either with phacoemulsification(fig.1)Goniosynechioysis is performed with viscoelastic injection(fig.4)with spatula and with a forceps. Sutures are placed to the iris in order to make normal form size of the pupile, and widen the angle. (fig.1) (fig.2) (fig.3) (fig.4) (fig.5) (fig.6) (fig.7) (fig.8)
Clinical case Patient M.OD Angle-closure glaucoma.Mydriasisafteracute angleclosureattack. Plateau iris. BCVA= 0,6IOP –34,5mm Hg Patient M. OD in 2yearsafter operation BCVA= 0,8IOP –16,5mm Hg
Patients and methods: In this retrospective study 168 eyes of 110 consecutive patients with medically uncontrolled chronic ACG underwent ACA reconstruction. Mean age of patients was 64.6 ± 14.4 years. There were 24 men and 86 women. Mean preoperative IOP was 40.8 ±17.51 mmHg, mean visual acuity was 0.34 ±0.30. Patients were observed n day 3, months 1, 3, 6, 12, , 24, 48 after operation. The 6 months results were obtained in 168 cases, in terms more than 1 year in 125, more than 24 months in 72 cases. All the patients were on two or more antiglaucoma medications. Laser iridotomy was performed in 96 eyes before operation. Results: Mean follow up was 18.7±2.4 months. No antiglaucoma medications were used after surgery. Dynamics of IOP and visual acuity was the following. On day 3 after operation mean IOP was 19.10± 4.42 mmHg, mean visual acuity 0.42±0.22; one month 20.54±3.53, 0.47±0.24, three months 20.52±3.44 , 0.66±0.16; half year 20.14±4.53 , 0.56±0.28, one year 20.24±2.49 , 0.50±0.26, two year and a half 20,95±3,53, 0,65±0,31 respectively. The efficacy of the method was 94 % without medications after 1 year. The efficacy after 2 years - 92 % without medications. (96 % with antiglaucoma medications) (98 % with antiglaucoma medications) Conclusions: The developed technology of chronic angle-closure glaucoma treatment proved to be safe and effective.