Download
1 / 9
100 likes | 390 Views
Zonular Weakness in Patients with Primary Angle-Closure Glaucoma Yong Yeon Kim 1 , Keny Kirti 2 , Bokun Rho 1 Department of Ophthalmology, Korea University College of Medicine, Seoul, Korea 1 Department of Ophthalmology, Mumbai University, Seth G.S. Medical College, Mumbai, India 2

E N D
Zonular Weakness in Patients with Primary Angle-Closure Glaucoma Yong Yeon Kim1, Keny Kirti2, Bokun Rho1 Department of Ophthalmology, Korea University College of Medicine, Seoul, Korea1 Department of Ophthalmology, Mumbai University, Seth G.S. Medical College, Mumbai, India2 The author has no financial interests in this study
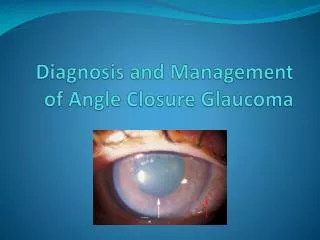
Purpose To evaluate the incidence of zonular weakness when primary angle-closure glaucoma patients underwent subsequent cataract surgery
Methods I • Retrospective study of 91 patients • The primary angle-closure glaucoma group: 26 eyes of 26 patients with subsequent development of cataract • The control group: 65 eyes of 65 patients with no other ocular problems except for cataract • Exclusion criteria: history of ocular trauma, ectopia lentis (homocystinuria, Marfan syndrome), pseudoexfoliation
Methods II • Patients in both groups underwent cataract surgery by the phacoemulsification technique through a temporal corneal incision bythe same surgeon • Zonular weakness was determined intraoperatively and confirmed postoperatively by review of video
Methods III • Zonular weakness was considered to be present when multiple sinusoidal folds formed during continuous curvlinear capsulorhexis at the tip of the capsulorhexis needle or forceps Illustration of the formation of sinusoidal folds. Curved lines outside the lens represent loosened zonules, and straight lines outside the lens represent intact, tight zonules Sinusoidal folds formation. When the zonule is loose, it cannot stretch the anterior capsule tightly, and the operator can find sinusoidal folds in the direction of the tip of the capsulorhexis needle or forceps
Results I Table 1. Demographic data and the patient characteristics PACG: primary angle-closure glaucoma IOP: intraocular pressure * Fisher’s exact test †T- test
Results II Table 2. Distribution of zonular weakness associated with other risk factors in angle-closure glaucoma patients PAS: peripheral anterior synechiae Hx: history CI: confidence interval * Fisher’s exact test † statistically significant
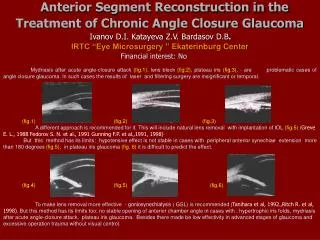
Discussion • Increased susceptibility to zonular weakness in cases of primary angle-closure glaucoma may be due to intraocular pressure related damage: sudden rise in intraocular pressure ischemia partial necrosis of iris stroma and ciliary processes instability of the ciliary complex forward displacement of the lens narrowing of angle and pupillary block • Iris atrophy found after angle closure attack in our study might be an indirect sign of ischemic insult to the ciliary complex
Conclusion • Zonular weakness was a significant finding in some cases of primary angle-closure glaucoma, especially when iris atrophy was present • The weakness may be due to ischemia from raised intraocular pressure, which damages the zonules and ciliary complex, or angle-closure attack itself may develop because of pre-existing zinular weakness