Download
1 / 49
500 likes | 930 Views
Development of the AORTIC ARCHES. Dr Rania Gabr. Objectives. Describe the formation of the aortic arches. Enlist the derivatives of aortic arches. Discuss the development of venous system of the heart. Differentiate between fetal and neonatal circulation.

E N D
Development of the AORTIC ARCHES Dr Rania Gabr
Objectives • Describe the formation of the aortic arches. • Enlist the derivatives of aortic arches. • Discuss the development of venous system of the heart. • Differentiate between fetal and neonatal circulation. • Discuss the congenital anomalies of the aortic arches.
Vascular Development——ARTERIAL SYSTEM Aortic Arches • During 4th and 5th weeks of development, aortic archesarise from aortic sac
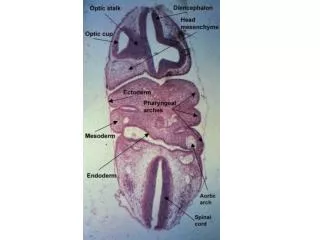
During folding: • The primitive aorta is divided into 3 segments: • Ventral aorta • First aortic arch • Dorsal aorta The 2 ventral aortae fuse to form the heart tube. Now the heart tube is connected to the dorsal aorta by the first aortic arch on each side.
The aortic arches terminate in right and left dorsal aortae. (In the region of the arches the dorsal aortae remain paired, but caudal to this region they fuse to form a single vessel.) Ventral view of the embryo Only the vessels on the left side of the embryo are shown.
aortic sac • The aortic aches appear in a cranial to caudal sequence gradually. • The aortic sac gives rise to a total of six pairs of arteries. During further development, some vessels regress completely. The fifth pair is rudimentary and disappears at a very early stage A. Aortic arches and dorsal aortae before transformation into the definitive vascular pattern.
Arch I: • By day 27, most of 1st aortic archhas disappeared on both sides, a small portion persists to form maxillary artery.
Arch II: • 2nd aortic archsoon disappears. • The remaining portions are hyoidand stapedial arteries.
Arch III:CAROTID ARCH – Persists becomes part of carotid arteries. • 1- Common carotid artery • 2-Proximal part of internal carotid artery • 3-External carotid artery
The remainder of internal carotid artery is formed by the cranial portion of the dorsal aorta
Arch IV:AORTIC ARCH -Right side: Rtsubclavian-Left side : Main Part of the ARCH OF AORTA. Arch V:DISAPPEARS
The aortic sac then forms right and left horns, which subsequently give rise to brachiocephalic artery and proximal segment of aortic arch, respectively. B. Aortic arches and dorsal aortae after the transformation. Broken lines, obliterated components. C. The great arteries in the adult.
Arch VI: PULMONARY ARCH – On the left side: Ventral part: Left pulmonary artery Dorsal part: Ductusarteriosus On the rtside:Ventral part: Right Pulmonary artery Dorsal part: Disappears ( No ductusarteriosus on the right side)
The left recurrent laryngeal nerve, recurs on the ductusarteriosus. • Absence of the ductus on the rt side allows the rt recurrent laryngeal nerve to recur on the rtsubclavian artery • Persistence of the Ductusarteriosus and later Ligamentumarteriosum is the cause of presence of the left recurrent laryngeal nerve in the thorax , while the rt remains in the neck due to absence of ductus on the rt side.
A number of other changes occur: • (a) dorsal aorta between entrance of 3rd and 4th arches, known as carotid duct, is obliterated. • (b) right dorsal aorta disappears between origin of the 7th intersegmental artery and junction with the left dorsal aorta.
So , the Arch of Aorta develops from 3 parts: • 1) Proximal part : from the left part of the aortic sac • 2) Middle part: from the left 4th aortic arch • 3) Distal Part: From the dorsal aorta between the left fourth and 6th arches
Vitelline Arteries • vitelline arteries, supplying yolk sac, gradually fuse and form arteries in dorsal mesentery of gut, celiac, superior mesenteric, and inferior mesenteric arteries. • These vessels supply derivatives of foregut, midgut, and hindgut respectively.
Umbilical arteries • The umbilical arteries are paired ventral branches of dorsal aorta • During the 4th week, each artery acquires a secondary connection with dorsal branch of aorta, common iliac artery, and loses its earliest origin. • After birth the proximal portions of umbilical arteries persist as internal iliac and superior vesical arteries, and distal parts are obliterated to form medial umbilical ligaments.
CLINICAL CORRELATES---Arterial System Defects • Under normal conditions the ductusarteriosusisfunctionally closed through contraction of its muscular wall shortly after birth to form the ligamentumarteriosum. • A patent ductusarteriosuseither may be an isolated abnormality or may accompany other heart defects. In particular, defects that cause large differences between aortic and pulmonary pressures may cause increased blood flow through the ductusarteriosus, preventing its normal closure.
Coarctationof aorta • It is a Local narrowing of the lumen of the aorta just distal to the origin of the Left SubclavianArtery ,above or below the entrance of ductusarteriosus. • 2 types: • In preductal type, ductusarteriosus persists • In postductal type, ductusarteriosus is obliterated.
Abnormal origin of the right subclavianartery(ABERRANT) • Right subclavian artery is formed by distal portion of the rightdorsal aorta and the 7th intersegmental artery. The right 4th aortic arch and proximal part of right dorsal aorta are obliterated. • With shortening of aortic arch, origin of abnormal right subclavian artery finally settles just below left subclavian artery. • Since its stem is derived from right dorsal aorta, it must cross midline behind esophagus to reach the right arm. This location does not usually cause problems with swallowing or breathing, since neither esophagus nor trachea is severely compressed.
Double aortic arch • right dorsal aorta persists between origin of 7th intersegmental artery and its junction with left dorsal aorta. • A vascular ring surrounds the trachea and esophagus and commonly compresses these structures, causing difficulties in breathing and swallowing. 7th intersegmental artery
Right aortic arch • left 4th arch and left dorsal aorta are obliterated and replaced by corresponding vessels on right side. • Occasionally, when ligamentumarteriosum lies on left side and passes behindthe esophagus, it causes complaints with swallowing.
common carotid arteries • Interrupted aortic arch • It is caused by obliteration of 4th aortic arch on left side. • It is frequently combined with an abnormal origin of right subclavian artery. • Ductusarteriosus remains open. • Descending aorta and subclavian arteries are supplied with blood of low oxygen content. • Aortic trunk supplies two common carotid arteries.
Development of Venous System • In 5th week of development 3 major pairs • Vitelline veins • Portal vein and superior mesenteric from right VV • Umbilical veins • Left umbilical vein connects to right hepatocardiac channel via ductusvenosus(bypass liver sinusoids) • After birth • Ductusvenosus closes ligamentumvenosum • Left umbilical vein is obliterated ligamentumtereshepatis • Cardinal veins main venous drainage of fetus
Cardinal veins (CV) • Ant. cardinal veins drain anterior region • Anatomose btw ant CV left brachiocephalic V • Post. cardinal V drain the rest • During 5th – 7th weeks more veins formed • Subcardinal V • Mainly drains the kidneys • Anatomose left renal vein • Supracardinal V • Drains the body wall by way of intercostal veins • Superior vena cava • From rt. common & proximal part of rt. ant. CV
Vena Cava, Azygous, Hemizygous • Superior vena cava • Formed by the right common CV & proximal part of right anterior CV • Inferior vena cava • Formed from right subcardinal vein • Azygous • Formed from right supracardinal veins • Hemizygous • Formed from part of left supracardinal veins
Fetal Circulation • By the third month of development, all major blood vessels are present and functioning. • Fetus must have blood flow to placenta. • Resistance to blood flow is high in the lungs.
Umbilical Circulation • Pair of umbilical arteries carry deoxygenated blood & wastes to placenta. • Umbilical vein carries oxygenated blood and nutrients from the placenta.
Umbilical vein to portal circulation • Some blood from the umbilical vein enters the portal circulation allowing the liver to process nutrients. • The majority of the blood enters the ductusvenosus, a shunt which bypasses the liver and puts blood into the hepatic veins .Then to Inferior vena cava
foramen ovale • Blood is shunted from right atrium to left atrium, skipping the lungs. • More than one-third of blood takes this route. • Is a valve with two flaps that prevent back-flow.
ductusarteriousus • The blood pumped from the right ventricle enters the pulmonary trunk. • Most of this blood is shunted into the aortic arch through the ductus arteriousus.
What happens at birth? • The change from fetal to postnatal circulation happens very quickly. • Changes are initiated by baby’s first breath.