Download
1 / 56
560 likes | 607 Views
Understand cellular growth adaptations, injury, and death mechanisms at sub-cellular levels. Explore concepts of apoptosis, necrosis, and cell aging, along with fatty change patterns and cell aging. Learn about cellular responses to maintain homeostasis and adaptations due to injuries.

E N D
CELL ADAPTATIONS CELL INJURY CELL DEATH DR.SAMINA QAMAR AP PATHOLOGY.
OBJECTIVES Understand the concepts of cellular growth adaptations---Hyperplasia, Hypertrophy, Atrophy, Metaplasia, Dysplasia Reversible, irreversible cell injury
OBJECTIVES Understand the pathologic mechanisms at the SUB-cellular level---ATP, Mitochondria, Ca++, Free Radicals, Membranes Understand and differentiate the concepts of APOPTOSIS and NECROSIS Understand SUB-cellular responses to injury---Lysosomes, Smooth endoplasmic reticulum, Mitochondria, Cytoskeleton
OBJECTIVES Identify common patterns of cellular swelling and fatty change. Cell aging
To maintain a steady state of structure and function is HOMEOSTASIS
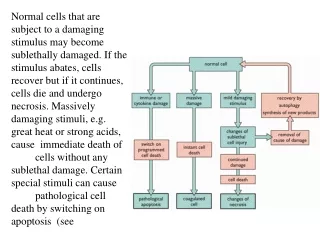
Cellular response to injury • Non-lethal injury: cell will adapt • Hypoxia, chemical injury, infection: Reversible injury will result in fatty change. Irreversible injury will result in death • Repeated Injury: cellular aging
ADAPTATIONS: Non-lethal injury. • Altered/changed steady state in structure and function of cell. • WHY: In response to physical/ pathological stimuli. Increased or decreased stimulation or any irritation.
The –plasia brothers • HYPER- • HYPO- (A-) • NORMO- • META- • DYS- • ANA- • “Frank” ANA-
HYPER-PLASIA IN-CREASE IN NUMBER OF CELLS, if they can divide.
The –trophy brothers • HYPER- • HYPO- (A-) • DYS-
HYPER-TROPHY IN-CREASE IN SIZE OF CELLS
A-TROPHY*? DE-CREASE IN SIZE OF CELLS? YES SHRINKAGE IN CELL SIZE DUE TO LOSS OF CELL SUBSTANCE
ATROPHY • DECREASED WORKLOAD • DENERVATION • DECREASED BLOOD FLOW • DECREASED NUTRITION • AGING (involution) • PRESSURE • “EXHAUSTION”
METAPLASIA • A SUBSTITUTION of one NORMAL CELL or TISSUE type, for ANOTHER • COLUMNAR SQUAMOUS (Cervix) • SQUAMOUS COLUMNAR (Esophagus) • FIBROUS BONE • WHY?
Examples: Respiratory epithelium, Barrett’s, myositis ossificans.
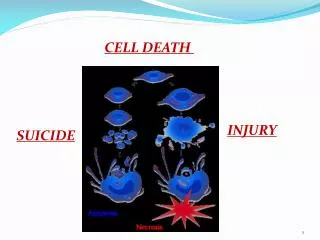
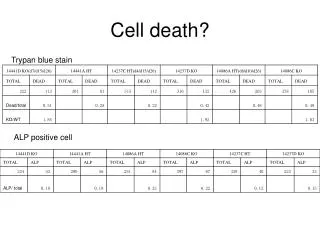
CELL DEATH What is DEATH? • DEATH is IRREVERSIBLE • But in cell its either reversible or irreversible. • APOPTOSIS vs. NECROSIS
REVERSIBLE CHANGES • REDUCED oxidative phosphorylation • ATP depletion • Cellular “SWELLING”
IRREVERSIBLE CHANGES • MITOCHONDRIAL IRREVERSIBILITY • IRREVERSIBLE MEMBRANE DEFECTS • LYSOSOMAL DIGESTION
REVERSIBLE = INJURY IRREVERSIBLE = DEATH SOME INJURIES CAN LEAD TO DEATH IF PROLONGED and/or SEVERE enough
CELL DEATH • APOPTOSIS (“normal” death) programmed death. • NECROSIS (“premature” or “untimely” death
INJURY CAUSES (REVERSIBLE) Hypoxia, (decreased O2) PHYSICAL Agents CHEMICAL Agents INFECTIOUS Agents Immunologic Genetic Nutritional
CHEMICAL INJURY • “Toxic” Chemicals, e.g CCl4 • Drugs, e.g tylenol • Dose Relationship • Free radicals, organelle, DNA damage
INJURY MECHANISMS (REVERSIBLE) DECREASED ATP MITOCHONDRIAL DAMAGE INCREASED INTRACELLULAR CALCIUM INCREASED FREE RADICALS INCREASED CELL MEMBRANE PERMEABILITY
What is Death?What is Life? • DEATH is • IRREVERSIBLE MITOCHONDRIAL DYSFUNCTION • PROFOUND MEMBRANE DISTURBANCES LIFE is……..??? Till death hasn’t occurred.
DEATH:ELECTRON MICROSCOPY B-Microvillus incorporated in cell, Blebs extruded from cell. C- Mitochondrial swelling.
APOPTOSIS: falling off. • NORMAL (preprogrammed) • PATHOLOGIC (associated with Necrosis)
“NORMAL” APOPTOSIS • Embryogenesis • Hormonal “Involution” • Cell population control, e.g., “crypts” • Post Inflammatory “Clean-up” • Elimination of “HARMFUL” cells • Cytotoxic T-Cells cleaning up
“PATHOLOGIC” APOPTOSIS • “Toxic” effect on cells, e.g., chemicals, pathogens • Duct obstruction • Tumor cells • Apoptosis/Necrosis spectrum
APOPTOSIS MORPHOLOGY • DE-crease in cell size, i.e., shrinkage • IN-crease in chromatin concentration, i.e., hyperchromasia, pyknosis karyorhexis karyolysis • IN-crease in membrane “blebs” • Phagocytosis
SHRINKAGE/HYPERCHROMASIA Karryorhexis, karryolysis.
Damaged/necrotic cells can accumulate fat: Fatty change • Commonly occurs in Liver, heart. • Due to defective uptake, catabolism or secretion of lipid. • Severe fatty change can alter cellular structure and function. • Seen in diabetes, alcoholism, obesity.
LIPID LAW • ALL Lipids are YELLOW grossly and WASHED out (CLEAR) microscopically