Download
1 / 74
1.03k likes | 5.45k Views
Cervical Orthopedic Tests. Chapters 3 & 4. Tenderness Grading Scale. Grade I – mild tenderness to palpation Grade II – mild tenderness with grimace and flinch to moderate palpation Grade III – severe tenderness with withdrawal Grade IV – severe tenderness with withdrawal from noxious stimuli.

E N D
Cervical Orthopedic Tests Chapters 3 & 4
Tenderness Grading Scale • Grade I – mild tenderness to palpation • Grade II – mild tenderness with grimace and flinch to moderate palpation • Grade III – severe tenderness with withdrawal • Grade IV – severe tenderness with withdrawal from noxious stimuli
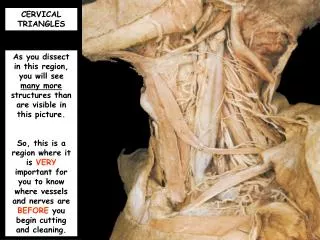
Cervical Palpation (Anterior) • Sternocleidomastoid • Carotid arteries • Supraclavicular Fossa
Cervical Palpation (Posterior) • Trapezius • Cervical intrinsic musculature • Spinous processes / facet joints
Cervical Range of Motion • Take a thorough history to be certain that these motions will not adversely affect the patient. • Trauma causing fracture, dislocation, or vascular compromise would be contraindications to performing these tests. • Note limited range of motion. • Note pain location and character.
Normal Cervical ROM • Flexion – 50 degrees or more • Extension – 60 degrees or more • Lateral flexion – 45 degrees or more • Rotation – 80 degrees or more
Cervical Resistive Isometric Testing • Evaluate muscle strength and state. • Weakness may indicate neurological dysfunction. • Pain indicates muscle dysfunction such as a strain.
Muscle Grading Scale • 5 – Complete range of motion against gravity with full resistance. • 4 – Complete range of motion against gravity with some resistance. • 3 – Complete range of motion against gravity. • 2 – Complete range of motion with gravity eliminated. • 1 – Evidence of slight contractility. • 0 – no evidence of contractility.
Vertebrobasilar Circulation Assessment • Vascular Insufficiency may be aggravated by positional change in the cervical spine. • Assessment of the vertebrobasilar circulation must be done if cervical adjustment or manipulation is to be performed.
Predispositions to Cerebrovascular Accidents • Headaches, migraine • Dizziness • Sudden severe head or neck pain • Hypertensive
Predispositions to Cerebrovascular Accidents • Cigarette smoking • Oral Contraceptives • Obesity • Diabetes
Cerebrobasilar Testing • Positional change in the cervical spine compresses the vertebral artery at the atlantoaxial junction on the side opposite of rotation. • In the normal patient, the diminished blood flow does not cause any neurological symptoms, such as dizziness, nausea, tinnitus, faintness, or nystagmus.
Clinical Signs and Symptoms of Cerebrovasular Episodes • Vertigo, dizziness, giddiness, light-headedness • Drop attacks, loss of consciousness • Diplopia • Dysarthria
Clinical Signs and Symptoms of Cerebrovasular Episodes • Dysphagia • Ataxia of gait • Nausea, vomiting • Numbness on one side of the face • Nystagmus
Barre-Lieou Sign • Procedure: Patient rotates head from one side to the other. • Positive Test: Vertigo, dizziness, visual blurring, nausea, faintness, nystagmus. • Structure affected: Vertebral artery on the same side of head rotation. Consider patency of the carotid arteries and the communicating cerebral artery circle.
Vertebrobasilar Artery Functional Maneuver • Procedure: Palpate and auscultate the carotid arteries for pulsations and bruits. Instruct the patient to rotate and hyperextend the head.
Vertebrobasilar Artery Functional Maneuver • Positive Test: If pulsation or bruits are present at either the carotid or subclavian arteries the test is positive. • Structures Affected: It may indicate stenosis or compression of the carotid or subclavian arteries.
Maigne’s Test • Procedure: Patient extends and rotates the head and holds that position for 15 – 40 seconds. Repeat on opposite side. • Positive Test: Vertigo, dizziness, visual blurring, nausea, faintness, and nystagmus. • Structures Affected: Vertebral, basilar, or carotid artery stenosis or compression.
Dekleyn’s Test • Procedure: Patient supine, head off table. Instruct pt. to hyperextend and rotate head. Hold 15 to 30 seconds. Repeat opposite. • Positive Test: Vertigo, dizziness, visual blurring, nausea, faintness, and nystagmus. • Structures Affected: Vertebral, basilar, or carotid artery stenosis or compression.
Hautant’s Test • Procedure: Pt. Seated, eyes closed, extend arms to front with palms up. Pt. extend and rotate head. • Positive Test: Patient loses balance, drops arms, and will pronate the hands. • Structures Affected: Vertebral, basilar, or carotid artery stenosis or compression.
Underburg’s Test • Procedure: Pt. standing. Close eyes and assess equilibrium. Stretch arms and supinate hands. Then pt. marches in place. Then pt. extends and rotates head while marching. Then opposite side.
Underburg’s Test • Positive Test: Patient loses balance, arms drift, hands pronate. Vertigo, dizziness, visual blurring, nausea, faintness, and nystagmus. • Structures Affected: Vertebral, basilar, or carotid artery stenosis or compression.
Hallpike’s Maneuver • Procedure: Pt. supine with head extended off table. Support head and move it into extension. Then laterally flex and rotate. Hold 15 to 40 seconds. Repeat opposite. Then hang head in free hyperextension.
Hallpike’s Maneuver • Positive Test: Vertigo, dizziness, visual blurring, nausea, faintness, and nystagmus. • Structures Affected: Vertebral, basilar, or carotid artery stenosis or compression.
Clinical Signs and Symptoms of Cervical Strain or Sprain • Cervical and upper back pain • Cervical and upper back stiffness • Cervical and upper trapezius tightness • Reduced cervical range of motion • Cervical extensor spasm
Differentiating Between Strain and Sprain • Cervical strain is an irritation and spasm of the muscles of the cervical spine with or without partial muscle fiber tearing. • Cervical sprain is a wrenching of the joints of the cervical spine with partial tearing of its ligaments.
Categories of Strain • Mild: Slight disruption of muscle fibers with no appreciable hemorrhage and minimal amounts of swelling and edema.
Categories of Strain • Moderate: Laceration of muscle fibers with an appreciable amount of hemorrhage into the surrounding tissues and a moderate amount of swelling and edema. • Severe: Complete disruption of the muscle tendon unit, possibly with tearing of the tendon from the bone or a rupture of the muscle through its belly.
Categories of Sprain • Mild: Slight tears of a few ligamentous fibers. • Moderate: More sever tearing of ligamentous fibers but not complete separation of the ligament.
Categories of Sprain • Severe: Complete tearing of a ligament from its attachments. • Avulsion: A ligament that attaches to a bone is pulled loose with a fragment of that bone.
O’Donoghue’s Maneuver • Procedure: Patient seated. Put the cervical spine through resisted range of motion, then through passive range of motion. • Positive Test: Pain during resisted range of motion or isometric muscle contraction signifies muscle strain. Pain during passive range of motion may indicate a sprain of any of the cervical ligaments.
O’Donoghue’s Maneuver • Structures Affected: Cervical spinal muscles and/or cervical spinal ligaments. • Since resisted range of motion mainly stresses muscles and passive range of motion mainly stresses ligaments, you should be able to determine between strain and sprain or a combination thereof.
Spinal Percussion Test • Procedure: Patient seated. Head slightly flexed, percuss the spinous process and associated musculature of each cervical vertebrae with a reflex hammer.
Spinal Percussion Test • Positive Test: Local pain may be a fractured vertebra with no neurological compromise. Radicular pain may be a fractured vertebra with neurological compromise or a disc lesion with neurological compromise. A ligamentous sprain could also elicit pain upon percussion of the spinous processes.
Soto-Hall Test • Procedure: Patient Supine. Press on the patient’s sternum with one hand. With the other hand, passively flex the patient’s head to the chest. • Positive Test: Local pain could indicate ligament, muscular, ossous pathology or cervical cord disease. Suspect disc defect with radicular symptoms.
Rust’s Sign • Procedure: A patient with severe injury to the upper cervical spine will grasp the head with both hands to support the weight of the head on the cervical spine. The supine patient will support the head while attempting to rise. • Positive Sign: The patient stabilizes the head. It might include slight traction.
Rust’s Sign • Structures Affected: This could represent severe muscular strain, ligamentous instability, posterior disc defect, upper cervical fracture, or dislocation.
Cervical Instability Clinical Signs and Symptoms • Severe cervical pain. • Patient stabilizing the head. • Little or no cervical motion. • Severe cervical muscle spasm. • Upper extremity neurological dysfunction. • Lower extremity neurological dysfunction.