Download
1 / 13
160 likes | 840 Views
Heart failure. Heart failure, also called congestive heart failure, is a disorder in which the heart loses its ability to pump blood efficiently. Heart Failure. Causes of Heart Failure Coronary Artery Disease and Heart Attack High Blood Pressure Valvular Disease Other Concerns

E N D
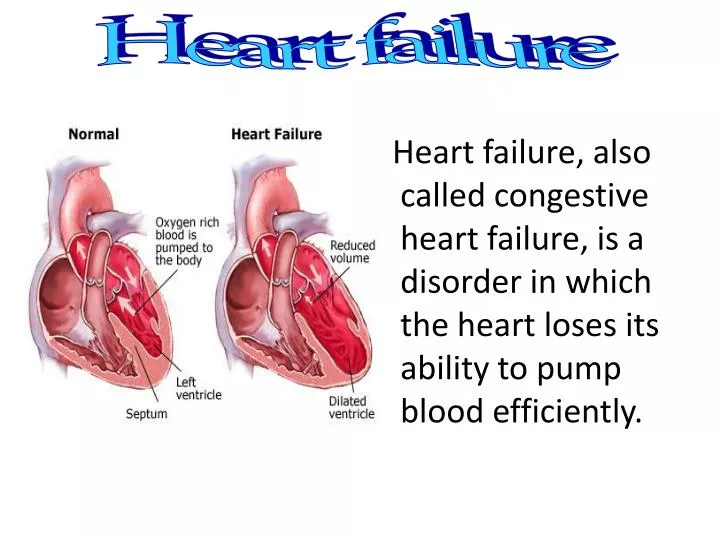
Heart failure Heart failure, also called congestive heart failure, is a disorder in which the heart loses its ability to pump blood efficiently.
Heart Failure Causes of Heart Failure • Coronary Artery Disease and Heart Attack • High Blood Pressure • Valvular Disease • Other Concerns a-Diabetes. Diabetes is linked to obesity, high blood pressure, and coronary artery disease. These conditions also can contribute to heart failure. b-Alcohol abuse. Too much alcohol can damage the heart muscle and lead to high blood pressure, which is also a risk factor for heart failure. symptoms 1-Edema leading to: • IN Tissues: Swelling of feetand ankle Swelling of the abdomen • In lungs: Shortness of breath Fatigue, weakness • 2-Decreased urine production • 3-Tachycardia
Compensatory mechanisms in heart failure Inadequate CO = decreased O2 delivery to tissues { So kidney and the brain get mad} • CO stimulate VMC & CAC in brain NE: from sympathoadrenal system reflex tachycardia + increases the after load (due to VC. of blood vessels) which requires the heart to do more work • CO decreased renal filtration pressure + increase in the sympathetic supply to kidney release reninangiotensin II aldosterone (increase in preload & after load ) • Enlarged heart and stretching in its muscle fibers: (mainly due to in angiotensen II & aldosteron) the heart enlarge, this eventually cause more weaking in heart. All these effects make the heart muscle itself become more and more weekend.
Heart Failure Diagnosis • medical history • Any symptoms you may have Also,to confirm a heart failure diagnosis: • Laboratory blood tests. • Chest X-Rays • Electrocardiogram (ECG)
Medications for Treating Heart Failure 1- Diuretics Most patients with heart failure require treatment with diuretics to relieve symptoms of fluid retention (edema and congestion), but their is no evidence that diuretics slow the progression of the disease or decrease mortality. • Loop diuretics (furosemide, bumetanide, torsemide) are the most effective diuretics • Thiazide diuretics (e.g. Hydrochlorothiazide ) act on the distal loop and are less effective than loop diuretics -The most serious adverse effect of diuretic therapy is potassiumdepletion (hypokalemia)as it can lead to arrhythmia which can be prevented by use of supplemental potassium or a potassium-sparing diuretic (spiranolactone which also heart remodeling)
2- Vasodilators a-Angiotensin-converting enzyme (ACE) inhibitors . Examples include enalapril , lisinopril and captopril . Mechanism of action : -ACEI inhibits Ag II formation (most pressor agent) VD. of BV. In pre- & after load -ACE inhibitors also inhibits the increase in aldosteron( Na &H2O retention as well as heart remodeling) - ACE is also responsible for the inactivation of bradykinin, so that inhibition of this enzyme also leads to increased bradykinin level which can act as a local vasodilator agent. Adverse effects: • · Dry cough (due to bradykinin)………not used in asthmatic pat. • · Loss of taste • · Severe hypotension • · Rash • · Angioedema (due to bradykinin)
b-Angiotensin II (Ag-II) receptor blockers These drugs, which include losartan and valsartan have many of the beneficial effects of ACE inhibitors, but they don't cause apersistent cough (they do not affect bradykinin metabolism). They may be an alternative for people who can't tolerate ACE inhibitors. c-Nitrates: Ex. Glycerol trinitrate & Isosorbidedintrate 1-These drugs are prodrugs which ultimately form NO, a powerful vasodilator· NO is capable of dilating all blood vessels ( pre- & after load ). 2-They can improve symptoms and reduce mortality, but the less effective than ACE inhibitors. Adverse effects of Nitrates: · Postural hypotension • Tolerance · Tachycardia (mild and brief, resolves quickly) · headache (central VD) · Flushing of the face
3-β-Blockers • Beta-blockers were widely considered to be contraindicated for patients with heart failure (due to its –veinotropic effect) ,only a decade ago, they are now considered first-line therapy for patients with mild to moderate heart failure • Beta-blockers are contraindicated in patients with asthma or severe bradycardia , AV heart block and sinus bradycardia, diabetes. Ex. Carvedilol: A nonselective beta-blocker with alpha1-adrenergic antagonist activity (vasodilator) ; this agent also possesses significant antioxidant properties which may be beneficial • - β blocking sympathetic effect on heart & kidney ( tachycardia & rennin angiotensin system) • - α1 blocking effect VD in blood vessels( pre -& after load )
4-Inotropic Drugs all of these drugs work by increasing the contractility of the heart. Bottom Line: ALL INCREASE Ca2+i.
A-Digitalis glycosides(cardiac glycosides) Digoxin is the most widely used preparation of digitalis glycosides, although digitoxin is also used Mechanism of Action • The cardiac glycosides partially inhibit the Na+/K+ -ATPase pump, which causes an increase in intracellular Na+, slowing the rate of the Na+/Ca++ exchang, and thereby causing an increase in intracellular Ca++ ,thus increasing contractile force and CO. • This increases in the force of contraction (positive inotropic effect), increases renal perfusion ( this why digoxin has diuretic effect in patients with CHF). • It decreases heart rate (negative chronotropic effect), and decreases AV node conduction velocity (indirectly by stimulating vagus nerve + its antiaderenergic effect) .
Summary: – It inhibits Na-K ATPase, leading to increase in: intracellular Ca, contractile force and CO – It increases Conduction rate through heart specially ventricles (if Toxicity occure ……arrhythmia) – But it decreases AV nodal conduction (via vagus & antiadrenergic effect) which can leads to bradycardia & heart block. -The increase in CO------- will cause decrease in sympathetic activity, Rennin Ang. System activity, cardiac load & cardiac remodeling & produce a diuretic effect.
Therapeutic effectiveness and toxicity of Digoxin depend on potassium levels • » Low potassium – leads to toxicity (arrhythmia) • » High potassium – leads to decreased effectiveness • –Adverse Effects& toxicity CNS: Headache, weakness, drowsiness, visual disturbances GI: GI upset, anorexia (as it stimulates CTZ in brain) CV:- Arrhythmias (due to hypokalemia treated with lidocaine and KCl solution) -Partial or complete heart block (due to its indirect vagal and antiaderenergic effects on AV node which is treated with atropine) -Fab fragment :Antibodies to digoxin to remove the excess free drug.
Other Inotropic drugs: b-Beta1-agonists Ex. Dopamine, dobutamine have been used to treat acute and chronic heart failure (arrhythmogenic) Dopamine (i.v.) is used in acute heart failure (cardiogenic shock) to increase blood pressure and increase cardiac output • Dobutamine is a somewhat selective beta1-adrenergic agonist that lacks vasoconstrictor activity and causes minimal changes in heart rate c-Phosphodiasterase inhibitors Ex. Amirnone & milrinone • They increase myocardial and vascular smooth muscle cAMP & c.GMP concentrations through inhibition of phosphodiesterase activity • These agents therefore increase cardiac contractility and cause VD of BV (reduce afterload and preload) • Their main side effect ………arrhythmogenic.





















