Download
1 / 25
250 likes | 392 Views
Culture Change in Multi-Facility Systems. Mary Tess Crotty, MA Genesis HealthCare Ed McMahon, Ph.D. Golden Living. ?. Culture Change. Quality. What do Culture Change and Quality Have in Common?. In small groups, introduce yourselves, and identify one or two things.

E N D
Culture Change in Multi-Facility Systems Mary Tess Crotty, MA Genesis HealthCare Ed McMahon, Ph.D. Golden Living
? Culture Change Quality What do Culture Change and Quality Have in Common? • In small groups, introduce yourselves, and identify one or two things
CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with CMS Culture Change Concepts
Culture Change & Baldrige Criteria • Focus on the resident • Employee engagement • Strategic planning • Process Improvement • It’s all about culture!
Organizational Definitions of Culture Change • GHC – since 2004: A great place to be – to visit, live and work • Person-centered care • Practices organized by People, Care and Environment • Golden Living – since 2002: Living Life to the Fullest • Resident-directed care • Practices organized by Resident-Driven Systems, Creating Community, Staffing, Self-Managed Work Teams, Environment
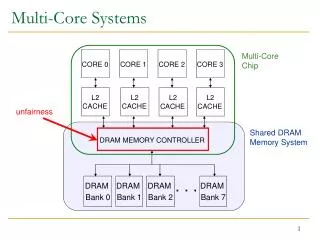
Right-Sizing Your Approaches • Genesis HealthCare • Approximately 220 nursing homes and assisted living centers, in 13 eastern seaboard states • operates in three geographical areas – 5-7 operations groups within geographical area • Collaborative Learning model – primarily by Area; monthly Conference Call companywide
Right-Sizing Your Approaches • Golden Living • Approximately 360, 22 states, 4 Divisions • Started with pilots and structured training • Integrated into companywide Performance Management System
Genesis Story • Collaborative Improvement Model • PCC materials developed by QIOs • Learning Sessions: area level Center team conferences, on-site learning sessions • Skill Development: Coaching Supervision (now The Partner Approach), Respectful Workplace Training, Neighborhood Training • Leadership Development
Genesis HealthCare The culture change story
Collaborative Improvement Model • Common goals and definitions • Learning sessions • Conference calls during “Collaborative work” periods • Final Congress
CMS/QIOs Collaborative • Pain Collaborative (Multi) • Workforce Retention (Multi) • Continued same format with Person-Centered Care (Culture Change)
Integrated into Quality Dept. • Common goals and definitions: • Culture Change Self-Assessments • Learning sessions • Range from 350+ - with direct care teams • Small pilots and on-site visits • Conference calls during “work” periods • Monthly Conference Calls (35-80 Centers) • Final Congress • Goals integrated into Customer Satisfaction, Employee Satisfaction/Retention, and Census
People Consistent Assignment Respectful Workplace/ Coaching Approach 3. Learning Circles 4. Orientation 5. Language Environment 12. Neighborhood Concept 13. Noise reduction 14. Safety and Independence Culture Change Assessment Areas Care • Medication Reduction • Bathing • Night-time Routines • Alarm reduction • Dining Choices • “Get to Know Me”-I Centered Care Plans
Self-Assessment Example: People 1. Consistent Assignments 1.1 Consistent Nurse Assistant assignments are in place for … M-F day shifts on (All/Most/Some/None) of the units. M-F evening shifts on (All/Most/Some/None) of the units. S-S shifts on (All/Most/Some/None) of the units. 1.2 The Center has a float/back-up system to provide consistent replacements. (Yes/No) 1.3 A team composed primarily of nurse assistants meets to discuss and oversee assignments… (Weekly/Monthly/Quarterly/Never) 1.4 Over the course of a month, a resident receives personal care from (No more than 10 NAs/Between 10 and 20 NAs/Over 20 NAs/Have no way of knowing) 1.5. Other Notes:
Culture Change Conferences Sample Themes… • Individualizing Daily Routines • Leading for Change • Patient Safety through Person-Centered Care • Creating Neighborhoods • The Spirit of Neighborhoods
Staff make most of the decisions with little conscious consideration of the impact on residents. Staff consult residents or put themselves in residents’ place while making the decisions. Resident preferences or past patterns form basis of decision making about some routines. Residents make decisions every day about their individual routines. When not capable of articulating needs, staff honor observed preferences and lifelong habits. Staff begin to organize their routines in order to accommodate resident preferences—articulated or observed. Staff organize their hours, patterns and assignments to meet resident preferences. Residents accommodate staff much of the time—but have some choices within existing routines and options. Residents accommodate staff preferences; are expected to follow existing routines. Continuum of Customer Orientation Low High Developed by Mary Tess Crotty, Genesis HealthCare Corp, based on the model by Susan Misiorski and Joanne Rader, distributed at the Pioneer Institutes, 2005.
InstitutionallyDirected InstitutionallyCentered Person Centered Person Directed Supervisors make most of the decisions with little conscious consideration of the impact on staff. Supervisors consult staff or put themselves in staff’s place while making the decisions. Workers’ make some decisions about how to arrange their routines to meet resident needs. Workers make decisions among themselves every day about how to arrange their routines to meet resident needs. Supervisors guide staff to organize their routines in order to accommodate residents. Supervisors oversee staff systems (hours, patterns, assignments) that workers create to meet resident preferences. Workers accommodate supervisor preferences; are expected to follow existing routines. Workers accommodate supervisors much of the time—but have some choices within existing routines and options. Continuum of Worker Orientation Low High
Conference Call Topics • I-Centered Care Plans • Noise Reduction • Bathing Options • Dining Approaches • Strengths-Based Approaches • Re-engineering the Med Pass • Self-Scheduling • Personal Alarm Reduction • Neighborhood Development
Skill Development • Used PHI (Sue Misiorski and colleagues), developed Train the Trainer model • Coaching Supervision (now The Partner Approach) – 2 day program for Department Heads and Nurses • Respectful Workplace Training • Neighborhood Training • Pilots (Resident-Staff Learning Circles, “Approach Coaches” for behavior challenges
Leadership Development • Rotating through Culture Change intensives by Operational Area – every other month, Administrators and DNSs attend an “onsite learning session” – within the company. • Integrating into our long-term care strategy for customer experience
Northeast Area 3 Yr Results • Coaching Supervision training • >1,800 completed 2-day training • Family Satisfaction • 1% increase to 90% would recommend • Employee Satisfaction • 9% increase to 70% would recommend • Occupancy • .6% decrease to 91.7%
Learning • Cultivate early adopters then recognize and reward them • Integrate into your discipline support • Bring leadership teams on-site to see and ask about change processes • Choose your framework – everyone needs to change – that takes time • Give concepts time to take root in your organization’s language • Be ready to adapt and connect culture change to organization’s priorities.
Golden Living The Culture Change Story