Download
1 / 9
90 likes | 288 Views
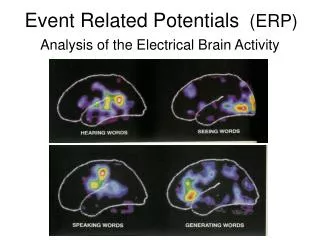
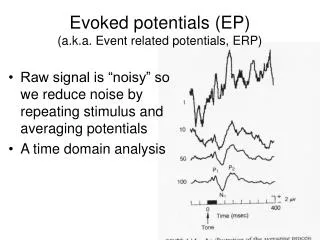
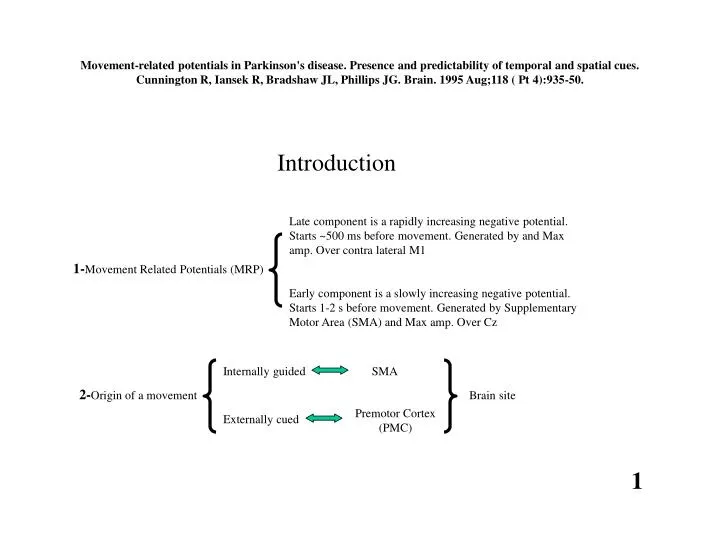
Late component is a rapidly increasing negative potential. Starts ~500 ms before movement. Generated by and Max amp. Over contra lateral M1. 1- Movement Related Potentials (MRP).

E N D
Late component is a rapidly increasing negative potential. Starts ~500 ms before movement. Generated by and Max amp. Over contra lateral M1 1-Movement Related Potentials (MRP) Early component is a slowly increasing negative potential. Starts 1-2 s before movement. Generated by Supplementary Motor Area (SMA) and Max amp. Over Cz Internally guided SMA 2-Origin of a movement Brain site Premotor Cortex (PMC) Externally cued Movement-related potentials in Parkinson's disease. Presence and predictability of temporal and spatial cues. Cunnington R, Iansek R, Bradshaw JL, Phillips JG. Brain. 1995 Aug;118 ( Pt 4):935-50. Introduction 1
4-PD patients have more problems with doing movement sequences. This problem with sequential movements is more pronounced than the problems PD patients have with simple movements or repetitive movement. Pooya: Although the problems of PD patients with sequential movements (in comparison with simple or repetitive simple tasks) is categorized as something distinct from their problems with internally guided (in comparison to externally triggered) tasks, I believe these are not distinct problems but the former is a manifestation of the latter. Because in doing a sequences of movements, one should internalize a larger load of information about the motion path in comparison to when they are going to do a simple or simple repetitive path. ! 3-SMA is in close relation to Basal Ganglia (BG). The function of SMA is disturbed in Parkinson’s Disease (PD), so PD patients have problems in internally guided movements and their early MRP is suppressed. Also PD patients show little tendency to internalize the control of an externally cued task, of which sequence can be predicted because of its repetitive nature. 5-A controversy: 1)When dealing with an internally guided sequential movement, SMA and BG are involved only in timing of sub-movements 2) SMA and BG are involved in preparation and processing of all the aspects of an internally guided sequential movement such as timing and movement direction, and target position. 2
! ! ! Pooya: Why not extinguished 4 s after the act of button depression was started? Therefore this temporal cue would have more validity and more accuracy in setting the pace of the action. Pooya: Here, internal means retrieved from memory. But there is also another situation that can be regarded as internal, that is decided by the person themselves. I like to study this variation too. Pooya: Size of the light board? Experiment one Methods: End Start 1-EEG recorded from Cz, sampled 100 Hz, low passed 20 Hz. Sweeps averaged from time –3 s to +1 s locked to each button release. Any sweep exceeding 150 micro volt in peak to peak amplitude was rejected as noisy. Each button was held down for 4 seconds before moving as fast as possible to the next button. patients were on drug. 21 patients and 21 normal age-matched subjects. 2-Internally cues versus externally triggered: cue absent versus cue present: In the former, people must pursue a memorized sequence and keep each button depressed for almost 4 seconds according to their own timekeeping system. In the latter, the path was illuminated when it was gone through (spatial cueing). Each button was extinguished extinguished 4 s after the release of the previous button (temporal cuing). 3
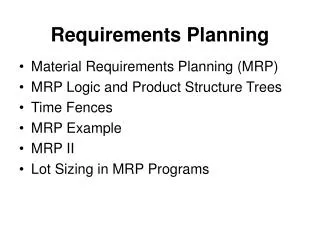
PD Cue absent normal Slope (micro volt/s) 8 -2s 0s PD= MRP peak at 0.1 s normals=0 s PD=late onset of early component ! ! 3 Pooya: Considering the fact that eye movements are congruent with hand movements when people point to buttons, this result is not what I expected. Pooya: Is this in contrast to the classic view toward PD that is recognized as overinhibition of motor cortes by BG? Cue present Cue absent Movement times in PD patients and normal controls are the same as each other, both around half a second. Pooya: patients were on drug. This explains why bradykinesia is not seen in their movements. But MRP features allegedly associated with PD bradykinesia (are still present in these patients. Does it mean that this alleged association should be reconsidered? ! PD normal Experiment one The slope of MRPs following the peak is less steep in PD than normals. Results: 10 micro volts This is because the pathologic Basal Ganglia is no longer able to terminate the activity of SMA as described by Watts & Mandir 1992. Also eye movements were recorded and no MRP was recorded correlated with eye movements. The bars show the slop of MRPs between –1.5 s and –0.5 s before each movement. This is the time window the early MRP is expected to be seen. As you see no early ERP is seen in PD patients in the cue present condition. Therefore, the rest of analysis is focused just on cue absent condition where both PD patients and normal subjects exhibit SMA activity evident by early MRP. As apparent in this figure, this MRP is less ample in PD patients. 4
Experiment three We saw in experiment one that in PD patients, presence of external cue turns off the SMA and absence of external cue results in some activity in SMA. The question here is that which aspect of the cue does this? The information it offers about the the spatial characteristics of the movement or those about the temporal characteristics of the movement? To approach this Q, 16 PD patients were recruited in this experimental setup: 5
Experiment three Results: 1-In this experimentin Parkinsonian patients, the absence and presence of early MRP cprrelates with presence and absence of temporal cueing and is not correlate with that of spatial cueing. 2-MRPs were not correlated with eye movements. 3-In PD patients, the internal control mechanisms operating via the supplementory motor area are only involved when no external timing cues are given and movements must be internally timed. 6
Experiment two 1-When externally cues are predictable, the control of the movement will be governed by internal predictory mechanisms. In this experiment, predictability of external cues are varied to see how the early component of MRP is affected. 2-This predictability is varied for the spatial cues and temporal cues distinctly to see whether the SMA is involved in just the timing of a movement or it is also involved in other aspects of motor planning like the direction of movement. 3-Ten normal subjects recruited. 7
Results: ! Pooya: It is worth noting that the most internal condition in experiment 2 (spatial and temporal cues both predictable) is the most external condition in Experiment 1 (cue present), Pooya: I do not agree with the authors that in this particular setup of experiment 2, when temporal cue is unpredictable the temporal control of movement is external. In contrast, I believe that it is very internal. Because in this situation the external cue is not informative about when the task should be done so subjects should ignore the external temporal cue and focus on what their internal clock says about whether the 4 s key press duration has elapsed or not yet. I would agree with the authors in that the unpredictable temporal cue is an external cue if the subjects were supposed to release the key in response to the presented temporal cue. ! Spatial Un/Predictability had no significant effect. Temporal Predictability= prominent Early MRP. Therefore SMA is involved in temporal but not spatial organization of internally controlled movements. Experiment two 8
Experiment four To make sure that our results were really due to activity in SMA the experiments 2 and 3 are replicated in 3 normal subjects and 3 PD patients with EEG recording from 9 sites on scalps. Most potent waves were recorded in Cz over SMA. 9