Download
1 / 1
10 likes | 118 Views
Persistence of Enophthalmos and Diplopia After Transconjunctival vs. Endonasal Repair of Orbital Blowout Fractures Hajirah Saeed MD, Shivani Kamat MD, Bruce Gaynes OD, Pharm D, David Yoo MD, Geeta Belsare Been MD Loyola University Medical Center, Maywood, IL. Research supported by :

E N D
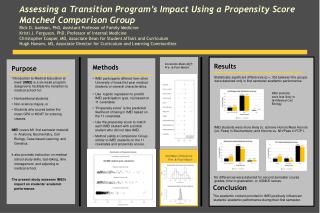
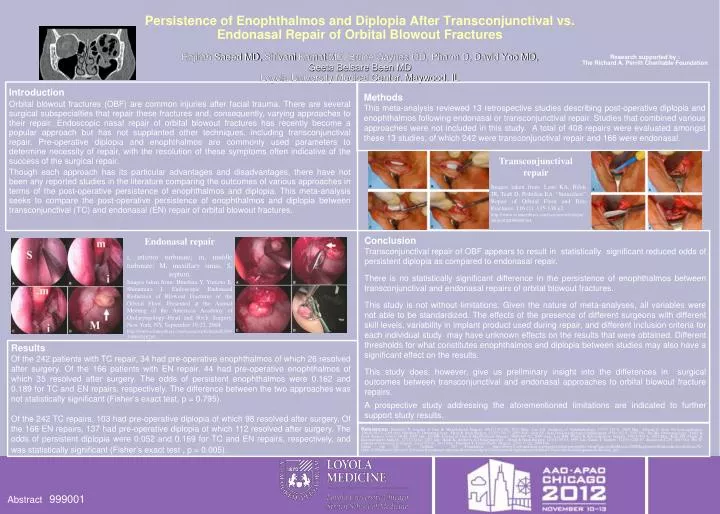
Persistence of Enophthalmos and Diplopia After Transconjunctival vs. Endonasal Repair of Orbital Blowout FracturesHajirah Saeed MD, ShivaniKamat MD, Bruce Gaynes OD, Pharm D, David Yoo MD, Geeta Belsare Been MDLoyola University Medical Center, Maywood, IL Research supported by : The Richard A. Perritt Charitable Foundation Introduction Orbital blowout fractures (OBF) are common injuries after facial trauma. There are several surgical subspecialties that repair these fractures and, consequently, varying approaches to their repair. Endoscopic nasal repair of orbital blowout fractures has recently become a popular approach but has not supplanted other techniques, including transconjunctival repair. Pre-operative diplopia and enophthalmos are commonly used parameters to determine necessity of repair, with the resolution of these symptoms often indicative of the success of the surgical repair. Though each approach has its particular advantages and disadvantages, there have not been any reported studies in the literature comparing the outcomes of various approaches in terms of the post-operative persistence of enophthalmos and diplopia. This meta-analysis seeks to compare the post-operative persistence of enophthalmos and diplopia between transconjunctival (TC) and endonasal (EN) repair of orbital blowout fractures. Methods This meta-analysis reviewed 13 retrospective studies describing post-operative diplopia and enophthalmos following endonasal or transconjunctival repair. Studies that combined various approaches were not included in this study. A total of 408 repairs were evaluated amongst these 13 studies, of which 242 were transconjunctival repair and 166 were endonasal. Transconjunctival repair Images taken from: Lane KA, Bilvk JR, Taub D, Pribtikin EA. “Sutureless” Repair of Orbital Floor and Rim Fractures. 116 (1): 135-138.e2 http://www.sciencedirect.com/science/article/pii/S0161642008008361 Endonasal repair i, inferior turbinate; m, middle turbinate; M, maxillary sinus; S, septum. Images taken from: Hinohira Y, Yumoto E, Shinamura I. Endoscopic Endonasal Reduction of Blowout Fractures of the Orbital Floor. Presented at the Annual Meeting of the American Academy of Otolaryngology–Head and Neck Surgery, New York, NY, September 19-22, 2004. http://www.sciencedirect.com/science/article/pii/S0194599805016293 Conclusion Transconjunctival repair of OBF appears to result in statistically significant reduced odds of persistent diplopia as compared to endonasal repair. There is no statistically significant difference in the persistence of enophthalmos between transconjunctival and endonasal repairs of orbital blowout fractures. This study is not without limitations. Given the nature of meta-analyses, all variables were not able to be standardized. The effects of the presence of different surgeons with different skill levels, variability in implant product used during repair, and different inclusion criteria for each individual study may have unknown effects on the results that were obtained. Different thresholds for what constitutes enophthalmos and diplopia between studies may also have a significant effect on the results. This study does, however, give us preliminary insight into the differences in surgical outcomes between transconjunctival and endonasal approaches to orbital blowout fracture repairs. A prospective study addressing the aforementioned limitations are indicated to further support study results. Results Of the 242 patients with TC repair, 34 had pre-operative enophthalmos of which 26 resolved after surgery. Of the 166 patients with EN repair, 44 had pre-operative enophthalmos of which 35 resolved after surgery. The odds of persistent enophthalmos were 0.162 and 0.189 for TC and EN repairs, respectively. The difference between the two approaches was not statistically significant (Fisher’s exact test, p = 0.795). Of the 242 TC repairs, 103 had pre-operative diplopia of which 98 resolved after surgery. Of the 166 EN repairs, 137 had pre-operative diplopia of which 112 resolved after surgery. The odds of persistent diplopia were 0.052 and 0.169 for TC and EN repairs, respectively, and was statistically significant (Fisher’s exact test , p = 0.005). References:Scolozzi P. Journal of Oral & Maxillofacial Surgery. 69(5):1415-20, 2011 May.; Lee CS. Archives of Ophthalmology. 127(3):291-6, 2009 Mar.; Schmal F. Acta Oto-Laryngologica. 126(4):381-9, 2006 Apr; Hinohira Y. Otolaryngology - Head & Neck Surgery. 133(5):741-7, 2005 Nov.; Jeon SY. Acta Oto-Laryngologica Supplement. (558):102-9, 2007 Oct.; Jin HR. Otolaryngology - Head & Neck Surgery. 136(1):38-44, 2007 Jan.; Jin HR. Journal of Oral & Maxillofacial Surgery. 58(8):847-51, 2000 Aug.; Lee HM. Plastic & Reconstructive Surgery. 109(3):872-6, 2002 Mar.; Kim YH. Plastic & Reconstructive Surgery. 127(1):321-6, 2011 Jan.; Ikeda K. Archives of Otolaryngology -- Head & Neck Surgery. 125(1):59-63, 1999 Jan.; Sanno T. Surgery. 112(5):1228-37; discussion 1238, 2003 Oct. Wu W. Journal of Craniofacial Surgery. 22(2):537-42, 2011 Mar.; Hinohira Y. Facial Plastic Surgery. 25(1):17-22, 2009 Feb. Image top left, N. Gellrich. AO Foundation. https://www2.aofoundation.org/wps/portal/surgerymobile?showPage=redfix&bone=CMF&segment=Midface&classification=92-Orbit,%20Orbital%20floor%20fracture&treatment=operative&method=Open%20treatment&implantstype=Orbital%20reconstruction&approach=&redfix_url= 999001