Download
1 / 88
931 likes | 1.16k Views
ALZHEIMER IMMUNOTHERAPY. $1,5 billion : a good investment?. Debarge Valentin Fontaine Quentin Olivier Jérôme. 02-2009. Summary. I/ The deal. II/ Mechanism of Alzheimer’s disease. III/ Active immunisation. IV/ Passive immunisation. V/ Our opinion. I/ The Deal. I/ The Deal.

E N D
ALZHEIMER IMMUNOTHERAPY $1,5 billion : a good investment? Debarge Valentin Fontaine Quentin Olivier Jérôme 02-2009
Summary I/ The deal II/ Mechanism of Alzheimer’s disease III/ Active immunisation IV/ Passive immunisation V/ Our opinion
I/ The Deal JULY 2, 2009 www.jnj.com
I/ The Deal • Alzheimer Immunotherapy Program (AIP): = Elan’s interest in a collaboration with Wyeth (now Pfizer) to research, develop and commercialize selective products for the treatment and/or prevention of neurodegenerative conditions, including Alzheimer’s disease www.elan.com In 2008, Elan spent $113 million on AIP, partnered with Wyeth (now Pfizer), and estimated it would spend as much as $500 million on bapineuzumab and the rest of the portfolio over the next 3 or 4 years. Impossible for Elan NATURE BIOTECHNOLOGY VOLUME 27 NUMBER 8 AUGUST 2009
I/ The Deal Summer 2008: two more patients taking the multiple sclerosis drug Tysabri (natalizumab) had contracted a potentially fatal brain disease : progressive multifocal leukoencephalopathy These events combined to drive down Elan’s stock from more than 23€ to less than 10€ The J&J deal solves both problems http://fr.finance.yahoo.com/
What did J&J want ? « As of April 2009, J&J did not list any neurodegenerative programs in its pipeline. We believe that AIP gives us a significant opportunity to build a position in Alzheimer’s disease by getting access to a late- stage molecule* that has potential in delaying progression of Alzheimer’s disease.” J&J spokesman Srikant Ramaswami * bapineuzumab BioCentury, the Berstein report on biobusiness July 6, 2009 Page A22 of 37
I/ The Deal Transaction $885 M 18,4% Elan's capital $ 500 M IP Elan (AIP) Estimated at $500 M 49,9% Janssen AI's capital Royalties Under conditions BioCentury, the Berstein report on biobusiness July 6, 2009 Page A22 of 37
I/ The Deal Transaction J&J purchased 107.3 million Elan's shares at $8,241/share J&J also agreed not to acquire any more shares for the next five years Royalties : ONLY after J&J has earned profits from the AIP equal to its $500 M The program will remain partnered with Wyeth, which was acquired by Pfizer Inc (01/2009, $68 billion) BioCentury, the Berstein report on biobusiness July 6, 2009 Page A22 of 37
What’s the level risk for J&J ? Bapineuzumab IanSanderson, analyst at Cowen, New York, gives bapineuzumab a 50% likelihood of reaching the market, based on clinician surveys conducted by the investment bank. NATURE BIOTECHNOLOGY VOLUME 27 NUMBER 8 AUGUST 2009
What’s the level risk for J&J ? Bapineuzumab Probability of success estimated = 50 % < 80 % • Why ? • AN 1792 fail • Disappointing phase II results • « first in class » in CNS therapeutic area
What’s the level risk for J&J ? Active immunotherapy Fail of AN 1792 Only in phase 2 today If immunotherapy fails … No γ-secretase inhibitor No Abeta aggregation inhibitor Tau protein way non explorated Empty pipeline ! NATURE BIOTECHNOLOGY VOLUME 27 NUMBER 8 AUGUST 2009
Alzheimer's disease : background Leerink Swann analysis. Extrapolated from UN census and prevalence data from 2008 US Alzheimer's facts and figures
Alzheimer's disease drugs market • $ 6.0 billion in 2008 • $ 7.8 billion expected in 2011 NATURE MEDECINE VOLUME 12 NUMBER 7 JULY 2006
Alzheimer's disease costs The current direct and indirect cost of caring for the 4,5 million Americans with AD was at least $100 billion annually in 2006 and estimated at $160 billion in 2010 Medicare costs Medicaid costs NATURE MEDECINE VOLUME 12 NUMBER 7 JULY 2006
Are they alone on the target ? Solanezumab is the main competitor of bapineuzumab but the overall trial is anticipated to be completed in mid 2012
Alzheimer’s disease Disease or neurodegenerative progressive appearance of mnemonic disorders evolving towards: a syndrome aphaso-apraxo-agnosic syndrome progressive loss of nerve cells in the brain death Mécanismes Moléculaires dans les Démences Neurodégénératives Inserm-UM2-EPHE U710 La maladie d’Alzheimer : aspects moléculaires, diagnostiques et thérapeutiques Octobre 2009
Histological signs We observe two types of damage in the neocortex : Tau protein and neurofibrillary tangles=NFTs (intra-neuronal) Beta amyloid protein (Aß) and senile plaques (extra-cellular) Mécanismes Moléculaires dans les Démences Neurodégénératives Inserm-UM2-EPHE U710 La maladie d’Alzheimer : aspects moléculaires, diagnostiques et thérapeutiques Octobre 2009
Senile plaques = insoluble substance (Aß) which settles slowly and gradually +++ in the grey matter of the cerebral cortex This substance seems to be neurotoxic in particular for neurones involved in the intellectual functions (memory, reading, writing, language, visual recognition …) Amyloid cascade hypothesis Synthesis of Aß peptide Mécanismes Moléculaires dans les Démences Neurodégénératives Inserm-UM2-EPHE U710 La maladie d’Alzheimer : aspects moléculaires, diagnostiques et thérapeutiques Octobre 2009
Amyloid cascade hypothesis Synthesis of Aß peptide From APP to Beta Amyloid (Aβ) neurons grow 1 ) Amyloid precursor protein (APP) APP may help damaged neurons to repair themselves and may help parts of neurons to grow after brain injury APP sticks through the neuron's membrane neurons survive Alzheimer's disease by Frank Lee adapted from the National Institute on Aging (NIA)
Amyloid cascade hypothesis Synthesis of Aß peptide 2 ) Aβ is generated from APP : β-secretase cuts APP at an outside position of the cell γ-secretase cuts APP at an inside position of the cell membrane Alzheimer's disease by Frank Lee adapted from the National Institute on Aging (NIA)
Amyloid cascade hypothesis Synthesis of Aß peptide 3 ) Fragments clump together and are mixed with other molecules,neurons and non-nerve cells Senile plaques Alzheimer's disease by Frank Lee adapted from the National Institute on Aging (NIA)
Amyloid cascade hypothesis Normal brain = Aβ40 production > Aβ42 production However, the amyloid plaque in Alzheimer's disease = Aβ42 Aβ42 aggregation faster than Aβ40 Alzheimer's disease by Frank Lee adapted from the National Institute on Aging (NIA)
The amyloid cascade theory Acknowledgments at the time of the deal JOURNAL OF NEUROCHEMISTRY | 2009 | 110 | 1129–1134
Genes involved in AD Mécanismes Moléculaires dans les Démences Neurodégénératives Inserm-UM2-EPHE U710 La maladie d’Alzheimer : aspects moléculaires, diagnostiques et thérapeutiques Octobre 2009
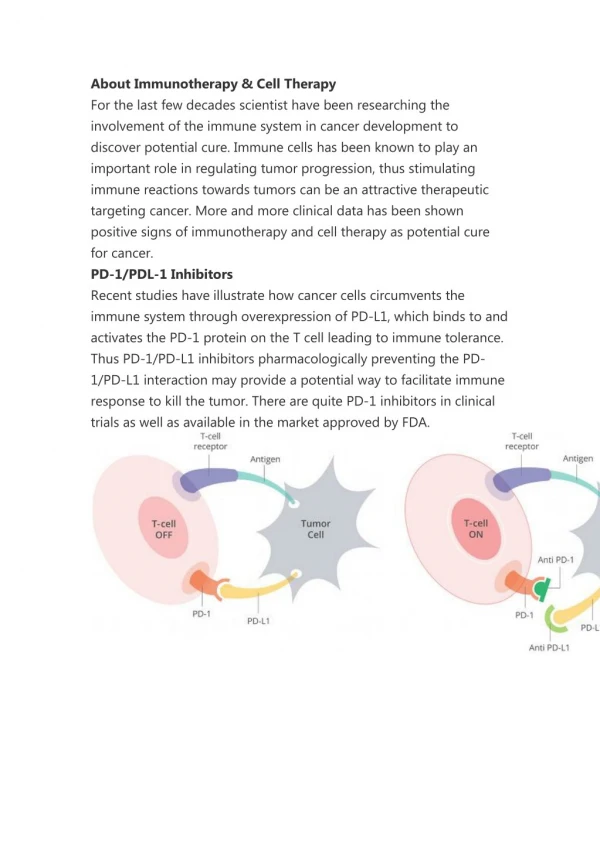
Generalities of immunotherapy ACTIVE: Injection of an antigen Production of antibodies PASSIVE: injection of antibodies directly Source:http://www.gensuisse.ch/gentech/mediz04_f.html
Beginning of Aβ42 immunisation Immunization with amyloid-β attenuates Alzheimer disease-like pathology in the PDAPP mouse Dale Schenk, Robin Barbour, Whitney Dunn, Grace Gordon,Henry Grajeda, Teresa Guido, Kang Hu, Jiping Huang,Kelly Johnson-Wood, Karen Khan, Dora Kholodenko,Mike Lee, Zhenmei Liao, Ivan Lieberburg, Ruth Motter,Linda Mutter, Ferdie Soriano, George Shopp, Nicki Vasquez,Christopher Vandevert, Shannan Walker, Mark Wogulis,Ted Yednock, Dora Games & Peter SeubertElan Pharmaceuticals, 800 Gateway Boulevard, South San Francisco, Amyloid-b peptide (Ab) seems to have a central role in theneuropathology of Alzheimer’s disease (AD). Familial forms ofthe disease have been linked to mutations in the amyloid precursorprotein (APP) and the presenilin genes. Disease-linkedmutations in these genes result inincreased production of the42-amino-acid form of the peptide (Ab42), which is the predominantform found in the amyloid plaques of Alzheimer’sdisease. The PDAPP transgenic mouse, which overexpressesmutant human APP (in which the amino acid at position 717 is phenylalanine instead of the normal valine), progressively develops many of the neuropathological hallmarks of Alzheimer’s disease in an age- and brain-region-dependent manner. In the present study, transgenic animals were immunized with Ab42, either before the onset of AD-type neuropathologies (at 6 weeks of age) or at an older age (11 months), when amyloid-b déposition and several of the subsequent neuropathological changes were well established. We report that immunization of the Young animals essentially prevented the development of b-amyloidplaque formation, neuritic dystrophy and astrogliosis. Treatment of the older animals also markedly reduced the extent and progression of these AD-like neuropathologies. Our results raise the possibility that immunization with amyloid-b may be effective in preventing and treating Alzheimer disease. Source:Nature 1999
Beginning of Aβ42 immunisation Principle Human Mutation APP717 Production of Beta amyloid plaques Source:http://www.gnis-pedagogie.org/pages/docbio/chap4/4.htm
Beginning of Aβ42 immunisation Results: Mouse immunised with Abeta 42 Human synthetic Transgenic Mouse with PBS
First human trial: AN1792 Elan pharmaceutical was the first in Active Immunotherapy on Alzheimer disease with AN1792 • PHASE I: 2000-2002 • 80 patients: 64 treated+16 placebo • 4 groups: 4 differentes formulations • AN1792 (50 or 225µg) with QS-21 adjuvant (50 or 100 µg) • Or QS-21only (control) in a 4:1 • Results: - One meningoencephalitis • - Good immune response Source:http://www.ncbi.nlm.nih.gov/pubmed/15883316?itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_RVDocSum&ordinalpos=1 http://www.neurology.org/cgi/content/abstract/64/1/94
First human trial: AN1792 AN1792:phase IIa Randomized, multicenter, placebo controlled, double-blind IM Evaluation of safety and tolerance 300 patients : 225μg of AN1792+ 50μg of QS21 72 patients : NaCl Immunisation: 0, 1, 3, 6, 9 & 12 months Patients with Alzheimer Disease MMSE 16 to 26 Age: 50 – 85 years 12 months rather than 15 as originally planned
Alzheimer’s tests on memory Mini Mental State Examination Referential test for inclusions The lower the score, the more sever the disease Only If people have equal access to treatment Orientation to time Naming ? • 30 : normal subject • 20-26 : mild AD • 15-19 : moderate AD Registration Reading Where are we ? Whatis the date today?
Results of AN1792 13/59 of responders 6% of meningoencephalitis 5/241 of low responders -No significant differences were found between antibody responder and placebo groups on battery of tests. -Only NTB test which revealed differences favoring antibody responders -CSF tau was decreased in antibody responders vs placebo subjects Source:-www.ncbi.nlm.nih.gov:80/pmc/articles/PMC2615484 -Neurology.2005 May 10;64(9):1553-62.Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial
Alzheimer’s tests on memory Neuropsychological Test Battery Long-term reminder memory test Memory span test Short-term & Long-term visual memory Verbal fluency language test 40’ Short-term & Long-term auditive memory Verbal learning test Acquisition test
Follow of AN1792 AN1792 stops in 2002, 1 year later, start « follow-up study » for 3 years. -Aβ42 immune response -degree of plaque removal -long-term clinical outcomes Obj: assess 80 subjects enrolled into phase I study Phase I study completed 44 patients dead or refusing consent for clinical follow-up 36 patients and/or carers agree to clinical follow-up and/or post mortem 10 patients died (10 treated) 26 patients alive (20 treated and 6 placebo) 12 patients treated 12 patients with placebo
Follow of AN1792 • Persistent elevated Antibody titers • No further cases of encephalitis • Aβ load: • -lower than in the unimmunised controls • -was considerable variation both in theAβ load andinthe degree of plaque removal among the immunised participants No correlation : Between anti-Aβ antibody titres at long-term follow-up and rate of decline as measured by at 6-year follow-up (ADAS-Cog;MMSE, or DAD)
Follow of AN1792 There is no significant amelioration of survival or evolution to severe dementia between AN1792 and placebo groups. However , the small numbers of participants enrolled in the initial study greatly limit the power of this study and a larger trial might have shown some small benefits that could not be detected with the cohort size examined here.
Conclusion for first immunotherapy tests Although immunisation with Aβ42 resulted in clearance of amyloid plaques in patients with Alzheimer’s disease, this clearance did not prevent progressive neurodegeneration. IMMUNOTHERAPY CAN BE ALWAYS A GOOD WAY FOR TREATMENT OF ALZHEIMER DISEASE?
Story continues with ACC-001 Principle • Nature of Ag: injection 7 amino acid fragment Abeta N-terminal • Supply:CRM197 (nontoxic variant diphteria toxin) • Adjuvant:QS21 (to stimulate immune response)
Story continus with ACC-001 First results • In April 2008 the ACC 001 phase II study was suspended because one patient developed a vascularitis resulting in skin lesions. • The cause is currently unknown Actually, this study is currently recruiting participants.
Story continus with ACC-001 Scheme of phase II Evaluating Safety, Tolerability, and Immunogenicity of ACC-001 in Subjects With Alzheimer's Disease Age: 50 – 85 years MMSE 16 to 26 ACC-001 + QS21 QS-21 is fixed at 50 micrograms. IM injection, dose 3-30micrograms, frequency: Day 1, month 1, 3, 6, &12. ACC-001 IM injection, dose 3-30micrograms frequency: Day 1, month 1, 3, 6, &12. QS-21: IM injection 50μg Drug: Phosphate buffered saline
Limits of Active immunisation approach: -The light immune response in older people -Trigger of chronic immune reaction and neurotoxic by T cell in the brain Also an other approach can be envisaged: PASSIVE IMMUNISATION
What is Bapineuzumab ? 1st humanized monoclonal candidate for AD Humanized version of the 3D6 murine monoclonal antibody Disulfide dimer between heavy and light chain of humanised mouse’s antibody AAB 001 IV phase III AAB 001 SC phase II Monoclonal Antibody Ig G1 Passive immunotherapie approach Target: the N-terminal 1-5 amino acids of Aβ peptides in amyloid plaques Goal: to bind to Aβ in the brain and facilitate its removal, yielding beneficial clinical effects http://www.alzforum.org/
Hypothesis on bapineuzumab’s activity Three mechanisms postulated: Direct effect of antibody on amyloid β Dissolution Neutralization of Aβ oligomers Amyloid β specific antibodies lead to Plaques with Fab domain Phagocytosis Microglial cells with Fc domain • The peripheralsinkhypothesis : Administration of amyloidβspecificantibodies • Efflux of Amyloidβfrombrain to blood Neurology 73 15 december,2009
Development of Bapineuzumab The phase 1 study One single ascending dose placebo controlled double blind study Primary outcome measures: safety-tolerability Secondary outcome measure: to characterize the pharmacokinetic Study’s design : 0,15 mg/kg or placebo 5,00 mg/kg or placebo • 54 patients • 50 to 85 years • MMSE 14-26 • Diagnosis of AD Results Safety and Tolerance 1,5 mg/kg dose demonstrated a significant increase in MMSE score The dose of 5,00 mg/kg was associated with MRI abnormalities in 3 out of 10 patients http://www.clinicaltrials.gov