Download
1 / 38
380 likes | 393 Views
This article discusses the burden of Alzheimer's Disease on individuals and society, the difference between normal aging and dementia, and the various stages of cognitive impairment. It provides valuable information for individuals living with dementia and their caregivers.

E N D
Living in the Community with a Diagnosis of Dementia Tara A. Cortes PhD,RN,FAAN Executive Director and Professor The Hartford Institute for Geriatric Nursing, NYU College of Nursing 2014 Primary Care Symposium June 9, 2014
Alzheimer’s Disease (AD) AD is different than other chronic diseases • There is no proven way to prevent it or modify its progression • It is strongly related to age • The rate of new cases doubles in each five year age group after age 65 • About 1 of 10 people over age 65 have AD • Almost 1 of 2 people over age 85 have AD • There is a need for supportive social care as cognitive abilities are lost resulting in caregiver burden • There is a financial burden due to high cost of medical care
Burden of Alzheimer’s Disease • Medical costs • Medications, doctor visits, hospitalizations • Almost all a burden to Medicare • Medicaid picks up direct costs for providing long term care in a nursing home or assisted living as people outlive their assets • Taxpayers become the payer
Burden of AD • Unpaid caregivers reduce the direct cost of long term supports • Indirect costs • Value of services provided by unpaid caregiver • replacement costs if those services had to be purchased • Caregiver reduces paid time in the workforce • Recent estimates of providing care for all patients over 70 is $157-$215 Billion estimated to rise to $1.2- $1.6 Trillion in 2040 (Hurd et al.)
Memory and Getting Older Normal Aging • As people get older they may forget things and remember them later • Forgetting the name of a person or object • Not knowing the day of the week • Sometimes needing help to change a setting on a TV or phone • Sometimes having trouble determining a tip • Trouble balancing a checkbook
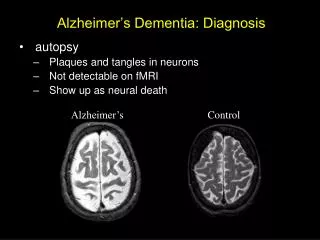
Dementia • Dementia affects about 5% of individuals 65 and older • Dementia describes the loss of memory and thinking that stops a person from doing their normal activities • AD is the most common type of dementia • Caused by changes that begin in the part of the brain that controls memory • These changes spread to other parts of the brain • Dementia can also be caused by vascular changes or other diseases, but AD is the cause of 60-80%
Dementia • Dementia is common in acute care and post-acute care facilities and their transitions, but under-recognized. • Symptoms of dementia can vary greatly, at least 2core mental functions must be significantly impaired to be considered dementia. • Individuals with clinically diagnosed dementia have clear cognitive loss in two or more intellectual domains but almost all individuals with Alzheimer's disease demonstrate short-term memory impairment. • Personality changes can become evident in the early stages of dementia. • Individuals with dementia may show symptoms of depression at any stage of the disease. Depression is treatable in the latter stages of dementia.
Normal Aging and Alzheimer’s Disease Typical Age Related Changes Alzheimer’s Disease Poor judgment and decision making Inability to manage budget Losing track of the date or season Difficulty having conversation Misplacing things and being unable to retrace steps to find them • Making a bad decision once in awhile • Missing a monthly payment • Forgetting which day it is and remembering later • Sometimes forgetting which word to use • Losing things from time to time
Alzheimer’s Disease • AD progresses from mild to moderate to severe cognitive decline • AD is a chronic disease that can go on for many years. • The usual time from diagnosis to death is between 8 and 15 years. • There is no cure but there are treatments that slow down the progression of the symptoms.
Mild Cognitive Impairment (MCI) • A person’s memory and thinking changes but they can still do all their normal activities • Changes are noticed over several months • Changes may include skills like: • Inability to balance check book • Trouble making change • Trouble choosing a tip • Searching for common words • The person continues normal ADLs such as driving, cooking dressing, shopping
Moderate Cognitive Impairment • Difficulty with decision making • Inability to recall own address or telephone number • Confused about where they are or what day it is • Unable to select appropriate clothes for season or occasion • Still independent in feeding and toileting
Severe Cognitive Impairment • Person may show personality changes and mood disorders, or delusions • May lose awareness of recent experiences and surroundings • Distinguish familiar and unfamiliar faces but have trouble remembering the name of a spouse and caretaker. • Need help dressing, toileting • May wander or become lost • May show compulsive behaviors like hand wringing or shredding tissues
Late Stage Alzheimer’s Disease • Individuals no longer respond to environment • Cannot carry on conversation • speak in single words or phrases • Need help with ADLs • eating, bathing, toileting • May lose ability to smile, sit without support or hold head up • Swallowing is impaired • Muscles grow rigid
Remember • It is difficult to place a person with Alzheimer's in a specific stage as stages may overlap. • Although usually considered a chronic disease of older adults, about 5-10% of people diagnosed with AD are <65 years of age. • Payment for care of this progressive disease can be challenging. • People with AD are at risk for abuse and neglect by others and themselves.
Concerns for Families and Loved Ones • Payment resources • Elder abuse • Caregiver burden • Resources for assistance • End of Life planning
Payment resources • Medicare • Does not pay for long term care • Pays for office visits, hospital care, short term rehab, home care for 60 days post hospital • Pays for hospice • Medicaid • Pays for long term care in home or nursing home • Must met income requirement
Elder Abuse • People with Alzheimer’s Disease are particularly vulnerable abuse and mistreatment • Caregivers — both family and professionals — are most often the abusers of older people. • In many cases, stress and frustration may provoke unintentional violent • There are different kinds of abuse • One sign of abuse may not be indicative, but repetitive signs must be taken seriously • Elder Justice Act • Part of the Affordable Care Act • Provides funds and grants to investigate sysematic abuse and stop it
Caregiver Burden • Caregivers of persons with Alzheimer’s disease and other dementias shoulder a particularly heavy burden of care. • Compared with other caregivers, the type of care they provide is more physically and emotionally demanding and more time-consuming, and it takes a heavier toll on work and family life.
Caregiver Burden • Family relationships change when Alzheimer’s strikes and intense caregiving occurs regardless of living arrangements. • Adult children are most often the primary caregiver, even when a spouse is present. • Most family caregivers do not live with the person for whom they are caring, but they still provide a great deal of care and support, even when their loved one is in a residential care facility.
Caregiver Burden • Alzheimer caregiving is about much more than activities of aily living (ADL). • Caregivers face special challenges arising from their loved ones’ cognitive impairment, and even more than other caregivers, they are addressing basic health care needs and struggling to negotiate the care system. • They are looking for information and help in carrying out these broader responsibilities.
Facts • 65% of caregivers provide the most difficult kinds of personal care – e.g. bathing, feeding and dealing with incontinence -- tasks that are even harder to do for a person with dementia who may be confused, disoriented, and unable to assist in even these most basic activities of daily living. • They spend more hours a week providing that care than do other caregivers. Nearly 1 in 4 provide what the survey defines as “constant care” – committing 40 hours a week or more. • They do so for a long time -- 71% for more than a year and 32% for five years or more. • Many spend substantial out of pocket expenses • Many work reduced hours or leave their jobs to provide care • In home care is expensive
More Facts • 20% to 30% of caregivers report they are prone to depression, grief, fatigue, and physical health problems • There is an increased use of alcohol, smoking and other drugs are not uncommon, as are poor health behaviors such as inadequate diet, exercise, and sleep. • Additional risks are a suppressed immune system leading to frequent infection and an increased risk of heart disease, diabetes, stroke and premature mortality. • Caregivers experience chronic conditions at nearly twice the rate of noncaregivers. • Although individuals who take on the caregiving role are generally physically healthier than those who do not, evidence suggests that at least one in ten caregivers report caregiving as the cause of their physical health's deterioration.
Reducing Burden • There is very little substantial research on reduction of stress in caregivers • Health professionals need to educate caregivers on care of older patients • Need to know when to call for help • The patient and caregiver must be perceived as a part of the healthcare team • Participate in health care plan • assure them that guidance is available to help in managing patient • Abandonment by the professional is most damaging as it makes the caregiver feel powerless
Reducing Caregiver Burden • The Reducing Disability in Alzheimer’s Disease (RDAD) program provides exercise training for people with Alzheimer’s disease who live at home and simultaneous training for their family caregivers about how to manage behavioral symptoms. • The program is intended to reduce behavioral symptoms and depression and improve the person’s physical functioning. • The RDAD intervention is 12 sessions over 11 weeks; each session is one hour in length. It could be done in-home or in-facility. It is designed to be delivered by professionals (not lay leaders) with experience guiding and supervising exercise activities in older adults. • Persons with dementia need to be living with a family caregiver or in a residential facility with caregiver staff that could guide and supervise the RDAD intervention.
Other Resources • Local support groups • Medical Day programs • PACE programs • Certified home health agencies • Medicaid • Hospice • Assisted living or nursing home • Alzheimer’s Association • 1-800-2723900 24 hour helpline • www.alz.org
End of Life Planning • More difficult when a patient has dementia • Includes a spectrum of decision making • Capacity • Health Care Proxy • POLST
Dementia and Capacity to Create an AD • If a patient with dementia can state the importance or implication of a choice on their future health state, they usually have the capacity to execute an AD • The ability to appreciate consequences is a highly valued standard for determining capacity to execute an AD • The capacity needed to name a proxy (e.g. execute a HCP) is less than that needed to execute a LW (Mezey, et al, 2000) • Patients with early dementia typically can safely execute a HCP • Patients with mild to moderate dementia typically lack capacity to execute an AD • However, these patients may be able to make or at least participate in some treatment decisions
Determining When a Patient Lacks Capacity Decision making capacity is a clinical determination • Competency is a legal determination • Criteria as to who can determine capacity varies across states
Determining When a Patient Lacks Capacity A patient lacks the capacity to make health care decisions when they cannot: • Understand and process information about their diagnosis, prognosis, and treatment options • Weigh the relative benefits, burdens and risks (e.g. consequences) of a care or treatment option • Apply a set of values to the analysis • Arrive at a consistent decision • Communicate the decision (Roth et al, 1977).
Standards for Proxy Decision Making • Voicing what the person said they would or would not want • Asking the proxy to make a decision the person said they would make for themselves • Making a decision that is in the person’s “best interest” • Ask the proxy if the patient made prior statements • Ask the proxy to make a decision based on what the patient would want if able to choose • Making a decision that a “reasonable person” would make
Health Care Proxy • Empowers a patient to name a proxy (surrogate) to make health care decisions if they lack capacity • Recognized in all states • A proxy can legally interpret the patient’s wishes to fit the actual situation • Thus, more flexible than a living will • Presumes that proxy knows the patient’s wishes • Not restricted to life sustaining treatment decisions • “Springing proxy”: can make decisions prn • Family consent laws • Web sources for HCP documents: google health care proxy forms and your state
POLST • Practitioner Orders for Life Sustaining Treatment • A set of orders to give seriously ill or frail older adults more control over their end-of-life care • Signed by MD/NP and patient/surrogate • New Jersey law requires that medical orders in a POLST be followed and provides immunity from civil or criminal liability to those who comply with it. • Complements Advance Directives which appoints a legal healthcare decision maker
POLST Document • Goals of care • Preferences regarding resuscitation • Preferences regarding intubation • Preferences for artificially administering nutrients • Other preferences regarding medical interventions that are unique to that patient
Palliative Care and Hospice Palliative Care Hospice Care Defined benefit under Medicare and most insurers Must have less than 6 months to live Must forgo curative care for illness that patient is admitted to hospice for Pays for all care related to illness including meds, equipment Bereavement care included for family post-death Can occur at home, nursing home, or time-limited stays in hospital • Empowers a patient to name a proxy (surrogate) to make health care decisions if they lack capacity • Recognized in all states • A proxy can legally interpret the patient’s wishes to fit the actual situation • Thus, more flexible than a living will • Presumes that proxy knows the patient’s wishes • Not restricted to life sustaining treatment decisions • “Springing proxy”: can make decisions PRN • Family consent laws • Web sources for HCP documents: google health care proxy forms and your state
PCP Management of Symptoms • Advance Care Planning: determine when to begin palliative care • Medicare billing allowed for palliative care evaluation and management • Determine patient’s values related to quality of life • Have patient complete an advance directive • Initiate symptom management • Move to Hospice
Policy Issues • It is essential that care for people with Dementia and AD be a policy priority • Economic burden on our system • Emotional, physical and financial burden of caregivers • The President has placed AD as a national agenda item • HHS is focused on AD with a national plan to have a cure by 2020
Public Policy Recommendations • Support the development of an essential infrastructure to serve family caregivers with a national accessible support system • After grant funding by Administration on Aging ends for successful programs, CMS should continue funding through waiver mechanisms • The CLASS Act (Community Living Assistance Services and supports Act) under the ACA should be re-introduced to support the development of a new national long term insurance program to include caregiver support, education and training.
There are only four kinds of people in this world. Those who have been caregivers, those who are currently caregivers, those who will be caregivers and those who will need caregiving. - Rosalyn Carter