Download
1 / 103
1.15k likes | 1.9k Views
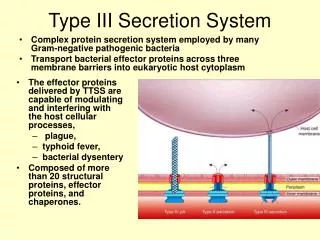
Pathogenic spirochetes: Borrelia. C hair of M icrobiology, V irology, and I mmunology. Groups of spiral shaped bacteria, which are pathogenic for human. Vibrio Campylobacter Helicobacter Spirilla Spirochetes Treponema Borrelia Leptospira. Evolution of spiral-shaped bacteria.

E N D
Pathogenic spirochetes: Borrelia. Chair of Microbiology, Virology, and Immunology
Groups of spiral shaped bacteria, which are pathogenic for human • Vibrio • Campylobacter • Helicobacter • Spirilla • Spirochetes • Treponema • Borrelia • Leptospira
Evolution of spiral-shaped bacteria Vibrio, Campylobacter, Helicobacter and Spirilla develop together with Eubacteria. Spirochetes are differed according to their morphological and physiological signs. There is hypothesis about their intermediate evolution position between Protozoa and Bacteria
Morphlogy of Campylobacter Comma-shaped form S-shaped form S-form Spiral-shaped form
Campylobacterjejuni 42oC 48h microaerophilic conditions
Main biochemical differences between Campylobacter andHelicobacter
Campylobacteriosis in human • Diarrhea (enterococlites), sometimes bloodly • Endoracditis, pericarditis, meningitis, encephalitis, septicemia • Disease of genitourinary tract • Pathology of pregnancy (abortion, premature delivery) • Autoimmune pathology with alteration of central nervous system
Helicobacter pylori History • In 1982 following the Easter holidays in the Microbiology Dept of the Royal Perth Hospital a culture of a spiral-shaped bacterium from gastric biopsies of patients with gastritis was isolated • The discovery was by Dr.Robin Warren and Dr.Barry Marshall • Noble Prize in 2005 • 2005 Nobel prize in 2005 • This discovery have revolutionised the diagnosis, treatment and prognosis of upper gastrointestinal disease • H. pylori causes gastritis in over half of the world`s population and is the aetiological agent of 95% of duodental ulcers, 70-80% of gastric ulcers and has casual rate in probably up to 60-70% of Gastric Cancer
H.pylori diseases in human • Chronic gastritis • Gastric and duodenal ulcer • Adenocarcinoma and B-Lymphoma of stomach • Alterations of cardiovascular system? Ulcerated gastric adenocarcinoma
Evidances of etiologic role of Helicobacter pyloriin pathogenesis of ulcer disease • > 95% patients with duodenal ulcer and > 80 % patients with gastric ulcer are infected with H. pylori: this level is more then in healthy persons; • In persons, which are infected with H. pylori, duodenal ulcer develops more frequently then in non-infected ones; • Antibacterial drugs have medicinal effect and safely prevent ulcer disease relapses
Peculiarities of Helicobacter pylori • Microaerophilic bacterium (5% О2, 5-10 % СО2); • They require special nutrient media, a surface of medium must be moist); • Selective medium required for isolation-10% sheep blood agar + selective antibiotic supplement They give growth in 48-72 hours, when antibiotics are used – in 13 days; • They have high urease, catalase and oxidase activity; • They are motile; • They are polymorphic bacteria (comma-shaped, spiral-shaped, coccal-shaped forms)
Pathogenesis of ulcer disease • Infection develops in antral part of stomach • Inflammation causes gastritis, duodenitis, but sometimes it is without any symptoms • Ulcer is result of inflammation,its complication - perforation and hemorrhage
Pathogenicity factors of H.pylori • Enzymes of virulence: • Urease • Phospholipase А • Proteases • Аdhesins • Toxins: • Endotoxin • Exotoxin-cytotoxin (factor which is responsible for formation of vacuoles)
Bacteriology • Catalase: antioxidant and protects from toxic oxygen metabolites from activated neutrophils • Protease: further degrade mucus • Phospholipase: alter phospholipid content of gastric barrier to change surface tension, hydrophobicity, and permeability • Receptor-mediated adhesion: Cag genes encode bacterial membrane proteins
Detection of vacuolizing factor in cell culture Positive results Negative results фактору
Survival factors of Helicobacter pyloriin a stomach • Neutralization of acidic contents of the stomachnear bacteria (urease, “altruistic autolysis”) • Active invasion in mucous layer which covers stomach epithelium (lophotrichates) • Ability to adhere to epitheliocytes of stomach (fimbria with hemagglutinin activity) • Micro-aerophilism – for survival within the mucous gel • Evasion of Immune response
Immune Response • Recall H Pylori is non-invasive but stimulates hearty inflammatory/immune response • Marked increase in platlet activation and aggregation: contribute to microvascular dysfunction and inflammatory cell recruitment • Antigenic substances: heat shock protein, urease, lipopolysaccharide (all activate T cells) • Cellular disruption at epithelial tight junctions enhances antigenic presentation • Increased IL-1, IL-6, TNF-alpha, and most notably IL-8 • IL-8: chemotactic, activates, recruits neutrophils
Immune Response • Also stimulates B cell response (IgG and IgA) locally and systemically (role of local antibodies unclear) • IgM antibodies: insensitive indicator of acute infection (and not clinically useful) • IgA and IgG remain present while infection active and decrease after infection cured • Antibodies to CagA protein detectable in gastric tissue and serum (more virulent organism)
Reservoir • Humans: major reservoir but seen in primates and domestic cats (may transfer to humans!) • Sheep: natural host? • H pylori seen in milk and gastric tissue • Higher infection rate in shepherds!
Transmission • Person to person: isolations of genetically identical strains from multiple family members • Fecal/oral: contaminated water in developing countries (h pylori can remain viable in water for several days) • Oral/oral: seen in dental plaque but prevalence is low • dentists don’t have higher prevalence • Iatrogenic infection: from endoscopes • GI docs/nurses increased risk for H pylori infection!
MODALITY ADVANTAGES DISADVANTAGES Endoscopy with Biopsy ( must be performed symtoms of Gastriccarcinoma or > 50Years) Permits inspection of pathology, allows detention of ulcers, neoplasms. Invasive, expensive, time consuming. Culture Performed in those Who have failed 2nd Line therapy Permits determination of antimicrobial susceptibilities and pathogenic features of isolates. Not optimally sensitive in most laboratories. Requires several days for results. Histology Generally more sensitive than culture. Allows direct visualisation of organism and extent and nature of tissue involvement. Gastritis may be patchy and biopsy may be performed on wrong area. Insensitivity to detect small numbers of organisms. Requires several days for results. Diagnosis
Urease Detection Rapid, most positives seen within 2 hours Increased sensitivity requires longer incubation. May be false positives with bacterial overgrowth. Serology Not reliable in young children Noninvasive, rapid, quantitative, inexpensive. No determination of lesions or pathology, no antimicrobial susceptibility. Not rapidly responsive to therapy. Urea Breath Tests 90% sensitivity and specificity Relatively non-invasive, relatively rapid, quantitative, rapidly responsive to therapy. Most valuable for assessing response to eradication therapy after 4-8 weeks. Involves expensive instrumentation or administration of radioisotopes. More invasive and less convenient than serology. No determination of lesions or pathology, no antimicrobial susceptibility. Diagnosis
Urease test for diagnosis of helicobacteriosis Test-system for diagnosis of helicobacteriosis
Standard triple therapy-Eradication therapy, which is probably the most widely used treatment for eradication of H. pylori.-7days mimimal Proton pump inhibitor B.D. (e/g Lansoprazole 30 mg BD) + Clarithromycin 500mg B.D. 1/52 90% plus effective + Amoxycillin 1g B.D. Or If penicillin allergic Proton pump inhibitor B.D. (e/g Lansoprazole 30 mg) Clarithromycin 500mgB.D. Metronidazole 400 mg B.D If treatment failure refer to Gasterenterologist
Rat-bite fever • A febrile, systemic illness usually acquired by direct contact with rats or small rodents • Streptobacillus moniliformis • Spirillum minor • Bites of lab rats are an increasing source of infection • Two distinct forms • “sodoku” – S. minus • Semticemia – S. moniliformis, epidemic arthriticerythema or Haverhill fever
Clinical manifestations are similar Both produce a systemic illness characterized by fever, rash, and constitutional symptoms Clinical differentiation is possible Semticemia – S. moniliformis, generalized morbilliform eruption to include palms and soles, may become petechial “sodoku” – S. minus, bite site is often inflamed and may become ulcerated Eruption begins with erythematous macules on the abdomen, which enlarge, become purplish red and forming extensive indurated plaques
Taxonomy • Order: Spirochaetales • Family: Spirochaetaceae • Genus: Treponema • Borrelia • Family: Leptospiraceae • Genus: Leptospira
General Overview of Spirochaetales • Gram-negative spirochetes • Spirochete from Greek for “coiled hair” • Extremely thin and can be very long • Tightly coiled helical cells with tapered ends • Motile by periplasmic flagella (a.k.a., axial fibrils or endoflagella) • Outer sheath encloses axial fibrils wrapped around protoplasmic cylinder • Axial fibrils originate from insertion pores at both poles of cell • May overlap at center of cell in Treponema and Borrelia, but not in Leptospira • Differering numbers of endoflagella according to genus & species
Spirochetes structure Cross-Section of Spirochete with Periplasmic Flagella NOTE: endoflagella, axial fibrils or axial filaments.
Spirochetes morphology Treponema Leptospira Borrelia
Spirochetes ultrastructure Borrelia Leptospira
Non-pathogenic T.denticola T.macrodenticum T.orale Conditionally pathogenic T.vincentii Pathogenic T.pallidum pallidum (syphilis) T.pallidum endemicum (bejel) T.pallidum pertenue (yaws) T.carateum (pinta) Classification of Human Treponema The treponemes responsible for these diseases cannot be distinguished serologically, morphologically, or by genome analysis, and they have not been successfully cultivated on artificial media.
Historical Background • Most accepted theory is that Christopher Columbus and his Crew brought back the bacteria which caused the disease Syphilis from the journey to the New World. • No distinctive signs of syphilis were found in Europe before he came back. http://www.solarnavigator.net/history/christopher_columbus.htm
Background Between 1905 -1910, Schaudinn & Hoffman identified T pallidum as the cause of syphilis The name "syphilis" was coined by Italian physician and poet Girolamo Fracastoro in his Latin written poem “Syphilis sive morbus gallicus” ("Syphilis or The French Disease") in1530
General Characteristics of Treponema pallidum • Too thin to be seen with light microscopy in specimens stained with Gram stain or Giemsa stain • Motile spirochetes can be seen with darkfield micoscopy • Staining with anti-treponemal antibodies labeled with fluorescent dyes • Intracellular pathogen • Cannot be grown in cell-free cultures in vitro • Koch’s Postulates have not been met • Do not survive well outside of host • Care must be taken with clinical specimens for laboratory culture or testing