Download
1 / 46
460 likes | 592 Views
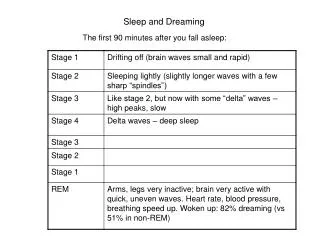
Obstructive Sleep Apnea: when dreams turn deadly. Troy Glembot, MD MBA CPE FACS FASMBS Medical Director Winchester Medical Center Bariatric Program. Objectives. Define OSA and identify its prevalence Identify patients who are at risk of having OSA Implications of untreated OSA

E N D
Obstructive Sleep Apnea: when dreams turn deadly Troy Glembot, MD MBA CPE FACS FASMBS Medical Director Winchester Medical Center Bariatric Program
Objectives • Define OSA and identify its prevalence • Identify patients who are at risk of having OSA • Implications of untreated OSA • Treatment options for patients who have OSA • OSA and potential safety issues in the workplace
Define OSA Sleep disordered breathing (SDB) Obstructive sleep apnea (OSA) Sleep apnea/hypopnea (SAH) Sleep apnea/hypopnea syndrome (SAHS) Obstructive sleep apnea syndrome (OSAS)
Obstructive Sleep Apnea • OSA is characterized by intermittent airway obstruction • Results in nocturnal desaturations hypercapnea • Increased inspiratory efforts lead to awakenings resulting in disturbed sleep
Epworth Sleepiness Scale From Johns MW: A new method for measuring daytime sleepiness: The Epworth Sleepiness Scale. Sleep 1991;14:540–545.
Obstructive Sleep Apnea Box 92-3. Diagnostic Criteria for the Obstructive Sleep Apnea-Hypopnea Syndrome The individual must fulfill criterion A or B, plus criterion C • Excessive daytime sleepiness that is not better explained by other factors • Two or more of the following (not better explained by other factors) • Choking or gasping during sleep • Recurrent awakenings from sleep • Unrefreshing sleep • Daytime fatigue • Impaired concentration • Overnight monitoring demonstrating five or more obstructed breathing events per hour during sleep; events may include any combination of obstructive apneas/hypopneas or respiratory effort-related arousals Adapted from American Academy of Sleep Medicine Task Force: Sleep-related breathing disorders in adults: Recommendations for syndrome definition and measurement techniques in clinical research. Sleep 1999;22:667–689.
Obstructive Sleep Apnea Principles of Sleep Medicine 2005
Prevalence of OSA • 4% of men and 2% of women have OSA • Prevalence peaks in men between 50-59 yrs. • Prevalence increases with older age in women Young et al, N Engl J Med 328: 1230-1235 1993
Prevalence of OSA • Ethnicity plays a role as well • Asian and Japanese patients have craniofacial geometries and smaller airway passages that may predispose OSA • African Americans typically have more severe OSA than whites even when adjusting for BMI, gender and age.
Prevalence of OSA What role does obesity play?
Prevalence of OSA BODY MASS INDEX BMI = Weight(kg)/Height(m)2 = (lbs./in.2)x 705
Prevalence of OSA BMI Indicators Acceptable Range 18.5 – 24.9 Overweight 25.0 – 29.9 Obese 30.0 – 34.9 Severe Obesity 35.0 – 39.9 Morbid Obesity 40.0 – 49.9 Super-Morbid Obesity > 50
Overweight Class I Obesity Class II Serious Obesity Class III Morbid Obesity BMI CHART (Sample Portion) Weight Height
Role of obesity in OSABRFSS, 1985 (*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person) No Data <10% 10%–14%
Role of obesity in OSA BRFSS, 2010 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
The Obesity Crisis • A Rapidly Expanding Problem • One in five people in the United States is obese • Three in five Americans are either overweight or obese • In the past 20 years, obesity among adults has doubled Source: The Surgeon General’s Call to Action to Prevent Overweight and Obesity.
Role of obesity in OSA http://www.google.com/imgres?q=bmi+and+obstructive+sleep+apnea&um=1&hl=en&biw=1280&bih=649&tbm=isch&tbnid=ev_aW35GBInbaM:&imgrefurl=http://journal.publications.chestnet.org/article.aspx%3Farticleid%3D1085729&imgurl=http://journal.publications.chestnet.org/data/Journals/CHEST/22068/zcb0100712270004.jpeg&w=1800&h=982&ei=CMlIUPzgE83GqAGz5oHYAw&zoom=1&iact=hc&vpx=933&vpy=368&dur=20240&hovh=166&hovw=304&tx=219&ty=148&sig=108640793115164267964&page=2&tbnh=95&tbnw=174&start=18&ndsp=24&ved=1t:429,r:17,s:18,i:184 accessed on 6 Sept 2012
Role of obesity in OSA Potentially life-threatening sleep apnea is unrecognized without aggressive evaluationHallowell et al, The American Journal of Surgery 193: 364-367. 2007 Expert Panel Recommendations Obstructive Sleep Apnea and Commercial Motor Vehicle Safety http://www.fmcsa.dot.gov/rules-regulations/TOPICS/mep/report/Sleep-MEP-Panel-Recommendations-508.pdf accessed on 6 Sept 2012
Role of obesity in OSA Expert Panel Recommendations http://www.fmcsa.dot.gov/rules-regulations/TOPICS/mep/report/Sleep-MEP-Panel-Recommendations-508.pdf accessed on 6 Sept 2012 Initially considered anyone with BMI > 30 kg/m2 to be screened for OSA over 41% of the drivers would need screened BMI cutoff raised to 33 kg/m2 , only 24% of drivers need screened
Implications of OSA So they snore
Implications of OSA Effect of apnea index on mortality * * * Cumulative survival * * Interval (years) Chest 88:9-14, 1988
Implications of OSA • CAD • ACS • Angina • HTN • Systemic HTN • Pulmonary HTN • Ventricular hypertrophy and dysfunction • Cardiac dysrhythmias • Bradycardia • Tachycardia • Atrial fibrillation • CVA
Implications of OSA • OSA is strongly linked to CVD • CAD appears associated with OSA • Up to 46% of patients presenting with an acute cardiac event had OSA • Moderately severe OSA (AHI > 20) is an independent risk factor for MI Skinner et al Chest 127(1): 2005 Schafer et al Cardiol 92(2): 79-84 1999
Implications of OSA • OSA is strongly linked to CVD • Hypertension appears exacerbated by OSA • Increased activation of sympathetic nervous system • Vascular endothelial dysfunction Somers et al J Clin Invest 96(4): 1897-1904 1995
Implications of OSA • OSA is strongly linked to CVD • OSA exacerbates CHF • Treatment of OSA results in improvement in LVEF and improved QOF on SF36 and chronic heart failure questionnaires. Kaneka et al, N Engl J Med 348(13): 1233-1244 2003
Implications of OSA • OSA is strongly linked to CVD • Almost 60% of patients with OSA have dysrhythmias • Both tachy and brady dysrhythmias • Up to 10% of patients develop transient heart block Hoffstein et al Chest 106: 466-471 1994 Harbison et al Chest 118: 591-595 2000
Implications of OSA • OSA is strongly linked to CVA • Up to 60% of stroke patients have OSA • The Sleep Heart Health Study demonstrated that OSA was associated with an increased prevalence of stroke Kaneko et al Sleep 26: 293-297 2003 Shahar et al Am J Respir Crit Care Med 163: 19-25 2001
Implications of OSA Sleep disordered breathing linked to apnea-induced hyperglycemia in diabetes • Nocturnal glucose values significantly higher in patients with OSA compared to those without OSA European Association for the Study of Diabetes meeting May 2007
Obstructive Sleep Apnea OSA isn’t just snoring • Think systemic….. Hypertension, ischemic heart disease, stroke, pulmonary hypertension, cor pulmonale, right heart failure
Implications of OSA • Over time, OSA gets worse Am J Respir Crit Care Med 2002;165:1217-1239
Implications of OSA The economic cost of sleep disordersSLEEP 2006;29(3):299-305 • Evaluation of the direct and indirect costs attributable to sleep disorders • Work related accidents, MVC, productivity losses
Implications of OSA SLEEP 2006;29(3):299-305
Implications of OSA SLEEP 2006;29(3):299-305
Implications of OSA • Untreated OSA adversely affects worker productivity • Excessive sleepiness, cognitive dysfunction, increased irritability and reduced vitality results in 30% reduction in productivity • Effect spans job salary levels American Academy of Sleep Medicine reported by New York Times June 14, 2011
Treatment • Lifestyle • Avoid alcohol, sedatives, sleep on your side, decongestants, quit smoking • Mouthpieces • Breathing devices (CPAP) • Surgery (UP3)
Treatment Am J Respir Crit Care Med 2002;165:1217-1239
OSA and workplace safety • Why would employers be concerned about OSA?
OSA and workplace safety • Happier employees • Untreated OSA is associated with depression and chronic fatigue
OSA and workplace safety • Happier employees • Untreated OSA is associated with depression and chronic fatigue • Healthier employees • Less time off work
OSA and workplace safety • Happier employees • Untreated OSA is associated with depression and chronic fatigue • Healthier employees • Less time off work • Less expensive • By keeping overall employee health optimized, heath care costs may be reduced
OSA and workplace safety • Untreated, OSA causes reduced psychomotor function, cognition which is directly related to accidents • MVC’s are particularly a concern J Clin Sleep Med 2009;5(6):573-581
Conclusions • OSA is a life threatening medical condition • Untreated OSA causes many other medical conditions • Untreated OSA is associated with increased health care costs and reduces worker productivity • Untreated OSA threatens worker safety • OSA can be effectively treated