Download
1 / 1
10 likes | 148 Views
Overall and 12 Week Tumor Response vs. Actual Tumor Measurements as Predictors of Overall Survival in Advanced Colorectal Cancer - Findings from NCCTG N9741 D.J. Sargent 1 , M Campbell 1 , A. Grothey 1 , R.M. Goldberg 2

E N D
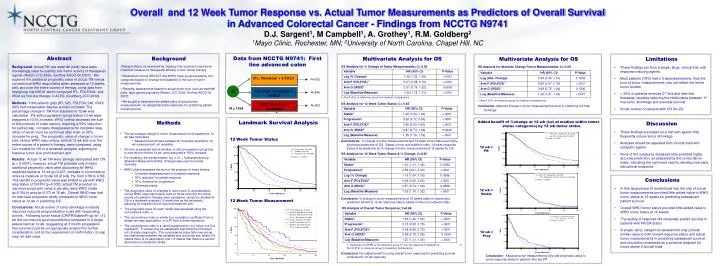
Overall and 12 Week Tumor Response vs. Actual Tumor Measurements as Predictors of Overall Survival in Advanced Colorectal Cancer - Findings from NCCTG N9741 D.J. Sargent1, M Campbell1, A. Grothey1, R.M. Goldberg2 1Mayo Clinic, Rochester, MN; 2University of North Carolina, Chapel Hill, NC Data from NCCTG N9741: First line advanced colon Abstract Background: Actual TM (via waterfall plots) have been increasingly used to quantify anti-tumor activity of therapeutic agents (Ratain JCO 2006, Grothey ASCO GI 2007). We explored the additional prognostic value of actual TM versus conventional WHO resp criteria when assessed at 12 weeks (wk) and over the entire course of therapy, using data from Intergroup trial N9741 which compared IFL, FOLFOX4, and IROX as first-line therapy in ACRC (Goldberg JCO 2004). Methods: 1164 patients (pts) (IFL 325, FOLFOX 546, IROX 293) had measurable disease and are included. The percentage change in TM from baseline to 12 wk was calculated. Pts with progression (prog) before 12 wk were assigned a 100% increase. WHO criteria assesses the sum of the products of index lesions, requiring a 50% reduction for partial resp, complete disappearance for complete resp, either of which must be confirmed after 4 wk, or 30% increase for prog. The prognostic value of change in tumor size, versus WHO resp criteria, both at 12 wk and over the entire course of a patient’s therapy, were compared, using Cox models for OS in a landmark analysis, adjusting for baseline tumor size and treatment arm. Results: Actual 12 wk TM were strongly associated with OS (p < 0.0001); however, actual TM provided only modest additional prognostic value after accounting for WHO response status at 12 wk (p=0.007, increase in concordance index (a measure of model fit) of only 1%, from 0.58 to 0.59). This benefit in prognostic value was limited to pts with WHO resp status of CR/PR (p=0.005); actual TM provided no improved prognostic value in pts who were WHO stable (p=0.35) or prog (p=0.57) at 12 wk. Overall WHO resp had no improved prognostic ability compared to WHO tumor status at 12 wk in predicting OS. Conclusions: Actual extent of tumor shrinkage modestly improves outcome prognostication in pts with responding tumors. Following tumor status (CR/PR/Stable/Prog) for >12 wk did not improve survival prediction compared to a single assessment at 12 wk, suggesting a) 3 month progression free survival could be an appropriate endpoint for further consideration, and b) the requirement of confirmation of resp may not add value. • Background • Disease status, as assessed by imaging, has long been used as an imperfect measure of therapeutic efficacy of anti-cancer therapy • Established criteria (RECIST and WHO) have grouped patients into categories based on change from baseline of the sum of tumor measurements • Recently, assessments based on actual tumor size, such as waterfall plots, have gained popularity (Ratain, JCO 2006, Grothey ASCO-GI, 2007) • We sought to determine the added value of actual tumor measurements, vs categorical tumor response, for predicting patient overall survival Multivariate Analysis for OS OS Analysis for % Change in Tumor Measurements; C= 0.63 1-Arm A (IFL) is reference group for treatment comparisons. OS Analysis for 12 Week Tumor Status; C= 0.65 Conclusions: % change in tumor measurements and 12 week tumor status are highly significant predictors of OS. Based on the concordance index, 12 week response status is as predictive as % change in tumor measurements at 12 weeks for OS OS Analysis for 12 Week Tumor Status & % Change; C=0.65 Conclusion: % change in tumor measurements at 12 weeks adds no meaningful prediction benefit to 12 wk response status, based on the concordance index OS Analysis of Overall Tumor Response; C=0.66 1- Response of CR/PR is the reference group for current response comparisons. 2- Arm A (IFL) is reference group for treatment comparisons Conclusion: No added benefit to using overall tumor response for predicting survival compared to 12 wk response Multivariate Analysis for OS OS Analysis for Absolute Change Tumor Measurements; C= 0.59 1-Arm A (IFL) is reference group for treatment comparisons. Conclusion: Absolute change in tumor measurements poorer in predicting OS than %change • Limitations • These findings are from a single, large, clinical trial, with response inducing agents • Most patients (75%) had ≤ 3 assessed lesions, thus the sum of tumor measurements may not reflect the entire tumor burden • > 50% of patients received 2nd line and later line therapies, possible reducing the relationship between 1st line tumor shrinkage and eventual survival • Small number of patients with CR (N=23) IFL: Irinotecan + 5-FU/LV N=325 R FOLFOX4: Oxaliplatin + 5-FU/LV N=546 IROX: Irinotecan + Oxaliplatin N=293 N = 1164 Landmark Survival Analysis 12 Week Tumor Status 12 Week Tumor Measurement Methods Added benefit of %change at 12 wk (cut at median within tumor status categories) by 12 wk tumor status • Discussion • These findings are based on a trial with agents that frequently induce tumor shrinkage • Analyses should be repeated from clinical trials with cytostatic agents • None of the measures assessed here provided highly accurate prediction, as assessed by the concordance index, indicating the continued need to develop new early clinical trial endpoints • The percentage change in tumor measurement from baseline to 12 wk was calculated • Measurement window between 8-16 weeks used when 12 wk measurement not available • Pts who progressed before window, or with progression (prog) due to new lesions before 12 wk, were assigned a 100% increase • For modeling, the transformation log (1.01 + %change) and log (Baseline Measurement/Abs. Change) was used to provide normality • WHO criteria assesses the sum of the products of index lesions • Complete disappearance for complete response • 50% reduction for partial response • 30% increase for progression • Otherwise stable • The prognostic value of changes in tumor size (% and absolute), versus WHO response criteria, both at 12 wk and over the entire course of a patient’s therapy, were compared, using Cox models for OS in a landmark analysis (12 week time as the landmark), adjusting for baseline tumor size and treatment arm. • The prognostic value for each model was assessed using the concordance index, c • The concordance index is similar to a correlation coefficient from a simple two-way association, or a R2 from a linear regression • The concordance index is a useful supplement to a p-value in a Cox regression. P-values may be statistically significant but the result not clinically meaningful. The concordance index tells how strong the relationship between the variables and outcomes are, where 0.5 means there is no association and 1.0 means that there is a perfect association or prediction ability. 12 wk = PR • Conclusions • In this large phase III randomized trial, the use of actual tumor measurements provided little added value to WHO tumor status at 12 weeks for predicting subsequent patient survival • Overall WHO tumor status provided little added value to WHO tumor status at 12 weeks • The quality of response did marginally predict survival in patients with PR/CR status • A single, early, categorical assessment may provide similar value to both overall response status and actual tumor measurements in predicting subsequent survival, and should be considered as a potential endpoint for future phase II clinical trials 12 wk = Stable 12 wk = Prog Conclusion: Absolute tumor measurements only add prognostic value to tumor response status in patients who are PR



















