Download
1 / 52
520 likes | 526 Views
Learn about toxicology, the science of poisons and the study of chemicals' adverse effects on living organisms. Explore the historical development, scope, and different types of toxic agents and toxicity. Discover the multidisciplinary nature of toxicology and its applications in clinical, forensic, environmental, analytical, and regulatory fields.

E N D
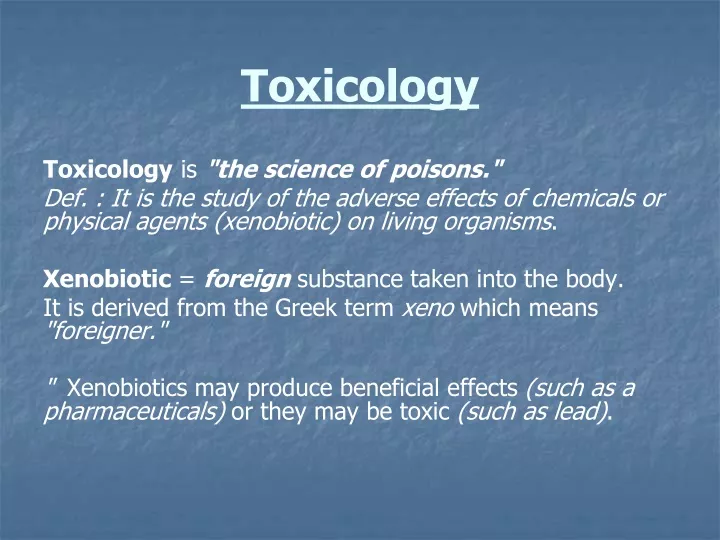
Toxicology Toxicology is "the science of poisons." Def. : It is the study of the adverse effects of chemicals or physical agents (xenobiotic) on living organisms. Xenobiotic = foreignsubstance taken into the body. It is derived from the Greek term xeno which means "foreigner." " Xenobiotics may produce beneficial effects (such as a pharmaceuticals) or they may be toxic (such as lead).
Historical Development of Toxicology It is one of the oldest practical sciences which began with early cave dwellers who recognized poisonous plants and animals and used their extracts for hunting or in warfare. By 1500 BC, hemlock, opium, arrow poisons, and certain metals were used to poison enemies or for executions (Notable poisoning victims include Socrates, Cleopatra, and Claudius) . The Death of Socrates, 1787 Jacques-Louis David (Metropolitan Museum of Art, New York)
By the time certain concepts fundamental to toxicology began to take shape especially by the studies of Paracelsus (~1500AD) and Orfila (~1800 AD). Paracelsus(1493 -1541): His famous words were : "All substances are poisons; there is none which is not a poison. The right dose differentiates a poison and a remedy." 1-He determined that specific chemicals were actually responsible for the toxicity of a plant or animal poison. 2-He also documented that the body's response to those chemicals depended on the dose received Orfila (founder of toxicology -19th century) Spanish physician who first correlated between the chemical and biological properties of poisons. The 20th century is marked by an advanced level of understanding of toxicology. DNA (the molecule of life) and various biochemicals that maintain body functions were discovered. Now our level of knowledge of toxic effects on organs and cells is being revealed at the molecular level.
Scope of Toxicology Toxicology is multidisciplinary as it entails: 1-Mechanistic Toxicology: Example: Biochemical toxicology: It deals with determination of mode of action of toxins at the molecular level. Behavioral toxicology: deals with the effect of toxin on the animal and human behavior (mainly on CNS & autonomic NS) Carcinogenesis: deals with the chemical and biochemical events that lead cancer. Teratogenesis: deals with the chemical and biochemical events that lead to deleterious effect on developmental process. Mutagenesis: it is concerned with toxic effect on the genetic material and the inheritance of these defects. 2-Applied Toxicology : Clinical Toxicology: It deals with emergency cases such as overdoses, poisonings, attempted suicides by: *Emergency care for patients. *Management of sign and symptom *Identification and quantification of the drug ,poisons, chemicals…etc .
Forensic Toxicology: It deals with medical-legal aspects of poisonings by: * Identification and quantification of poisons. * Establish relationship between tissue residual level and the cause of death. Economic Toxicology: It is concerned with development of drugs additives , food additives and pesticides. Environmental Toxicology: It is concerned with effects of different compounds on air, water and wildlife 3-Analytical Toxicology: It is concerned with quantitative & qualitative analysis of toxicant in body fluids, secretion and /or tissues. 4-Regulatory Toxicology: Risk assessment: It deals with analysis of toxicological data for the determination of: Safe level of drugs for humans , safe level of heavy metals in water , safe levels pesticides...etc. Legal aspect: Concerned with formulation of laws which are intended to minimize the effect of toxic chemicals on humans health & the environment.
Toxicity Def.: The degree to which a substance can harm humans or animal Different xenobiotics cause many types of toxicity by a variety of mechanisms.So, we have to take an idea about: -Different types of toxic agents -Different type of toxicity -Different mechanisms of toxic response
Toxic Agents Toxic agent: is anything that can produce an adverse biological effect. -The most common terms used to describe a toxic agent are toxicant, toxin, poison.
Toxic Agents are classified : 1-According to their nature: 1-Chemicals: as alcohols, phenols & heavy metals 2-Physical : as radiation. 2-Bilogical : Snake & scorpion venoms. 2-According to their effect: i-Systemic toxicant: is one that affects the entire body or many organs rather than a specific site. E.g.: potassium cyanide is a systemic toxicant in that it affects virtually every cell and organ in the body by interfering with the cell's ability to utilize oxygen. ii-Target organs toxicant: affect only specific tissues or organs while not producing damage to the body as a whole. Examples: -Arsenic& paracetamol are hepatotoxic. -Digitalis& antimony are cardiotoxic. -Mercury & gentamycin are nepherotoxic -Lead is also a specific organ toxin; however, it has three target organs (central nervous system, kidney, and hematopoietic system).
Types of poisoning Toxicity can be classified according to different variables as follow: 1-According to circumstances of poisoning: a-Accidental Toxicity (non-intentional poisoning): which occur by mistakes and usually happen to children (below 5-years old) E.g.:With aspirin, iron preparations, pesticides, kerosene…..etc. b-Deliberate self Toxicity (Suicidal or criminal poisoning): which occur when a person attempts to kill himself or another person. E.g.: with cyanide, barbiturates,salicylates…………………etc 2-According to incidence of poisoning: a-Homicidal:Which occurs in or around home. E.g.: pesticides, potassium hydroxide, disinfectants……. b-Occupational: This includes industrial and agricultural poisoning. E.g.: inhalation of pesticides.
Types of Toxicity 1-Systemic Toxicity : Toxicity may occur at multiple sites. This is referred as systemic toxicity. The following are types of systemic toxicity: -Acute Toxicity -Subchronic Toxicity -Chronic Toxicity -Carcinogenicity -Developmental Toxicity -Genetic Toxicity
a-Acute Toxicity: It occurs almost immediately (hours/days) after an exposure to single dose or a series of doses received within a 24 hour period. Death is a major concern in cases of acute exposures. Examples are: -In 1989, 5,000 people died and 30,000 were permanently disabled due to exposure to methyl isocyanate from an industrial accident in Bhopal, India. -Many people die each year from inhaling carbon monoxide from faulty heaters. b-Subchronic Toxicity: It results from repeated exposure for several weeks or months. This is a common human exposure pattern for some pharmaceuticals and environmental agents. Examples are: -Ingestion of coumadin tablets (blood thinners) for several weeks as a treatment for venous thrombosis can cause internal bleeding. -Workplace exposure to lead over a period of several weeks can result in anemia. c-Chronic Toxicity: It isa cumulative damage to specific organ systems and takes many months or years to become a recognizable clinical disease. This damage is so severe that the organ can no longer function normally and a variety of chronic toxic effects may result. Examples are: -Cirrhosis in alcoholics who have ingested ethanol for several years -Chronic bronchitis in long-term cigarette smokers -Pulmonary fibrosis in coal miners (black lung disease) d-Carcinogenicity: Carcinogenicity is a complex multistage process of abnormal cell growth and differentiation which can lead to cancer. e-Developmental Toxicity: Developmental Toxicity result from toxicant exposure to either parent before conception or to the mother and her developing embryo-fetus. f-Genetic Toxicity: Genetic Toxicity results from damage to DNA and altered genetic expression. This process is known as mutagenesis. The genetic change is referred to as a mutation and the agent causing the change as a mutagen.
2-Organ Specific Toxicity : Blood and Cardiovascular Toxicity Hypoxia due to carbon monoxide binding of hemoglobin preventing transport of oxygen Hepatotoxicity CCl4……..metabolized by HME…….CCl3 (causes lipid peroxidation in liver & lead to liver necrosis.) Nephrotoxicity Mercury & gentamycin are nepherotoxic. Neurotoxicity Organophosphorus compounds (insecticides)………damage to sensory fibers. Respiratory Toxicity Aluminum…..emphysema……inflated lung …….fibrosis(aluminosis). Dermal Toxicity dermal irritation due to skin exposure to gasoline dermal corrosion due to skin exposure to sodium hydroxide skin cancer due to ingestion of arsenic or skin exposure to UV light Eye Toxicity acids and strong alkalis may cause severe corneal corrosion corticosteroids may cause cataracts methanol (wood alcohol) may damage the optic nerve leading to blindness
Transported, dispersed, and possibly altered Ingested Contacts human Toxin emitted molecular mechanism Metabolized and/or stored Physiological chain of events Reaches an organ Adverse health effect Mechanism of Cellular Injury
Mechanism of Cellular Injury Toxicity can result from adverse cellular, biochemical, or macromolecular changes. Examples are: 1-Alteration of a cell membrane permeability: Toxic agents could change cell membrane permeability through interaction with its component as; a-SH-containing proteins: Heavy metals as As or Hg react with them……… change in protein structure ……… change membrane permeability. b-Lipids -Free radicals attack fatty acids in the lipid layer of biological membrane causing lipid peroxidation , these peroxides are toxic to the cell and alter membrane permeability. E.g.: CCl4……..metabolized by HME……CCl3 (Trichloromethyl radical causes lipid peroxidation and finally lead to liver necrosis.) -This is why antioxidants should be used frequently by humans where it act as a protective measure against many diseases(e.g.) Vit. E & Vit. C. c-Na-K ATPase pump: Many toxicants can inhibit these pumps which are essential for transport of major amino acids and calcium across the cell membrane. E.g.: Hg, Cu, Pb , As and alcohol .
2-Chang in enzyme activity: a-Inhibition: E.g.1: Carbamate esters (insecticides) reversibly inhibits anticholineserase leading to increase in A.Ch. Level Toxicity (SLUD are the most characteristic symptoms of toxicity). E.g.2: Cyanide………inhibits cytochrome oxidase enzyme……no aerobic respiration……….cell death. b-Activation: E.g.: Barbiturates induce hepatic microsomal enzymes increase the conversion of some non carcinogenic agents (in cigarette smoke) into carcinogenic ones. 3-Interferance with co-enzymes: E.g.: CN- binds to essential metals as Fe3+ needed for the activity of cyochrome oxidase. 4-Modification of carriers: E.g.1: CO binds with hemoglobin instead of O2 (affinity to Hb to CO is 210 times that for O2)……… carboxyhemoglobin…….hypoxia……death. E.g.2: Nitrates ,aspirin and sulfonamides oxidize Fe2+ in Hb into Fe3+ Hb …………………MeHb (methemoglobin) which can not carry oxygen NADPH-dependent Hypoxia MeHb reductase & Vit. C
5-Formation of reactive metabolites: E.g.: Benzo(α)pyrene metabolized by HME epoxide-7,8- dihydrodibenzo(α) pyrene Non-carcinogenic Carcinogenic In cigarette smoke 6-Reactions causing depletion of GSH: Glutathione (GSH) is an antioxidant which protects the cell from the harmful effect of oxidants. Reduction of GSH level into 20-30% causes impairment of cell defense mechanism . E.g.: N-acetyl-P-benzoquinone imine (NABQI) ,a toxic metabolite of paracetamol it is conjugated with GSH depletion of reduced form of GSH leading to NABQI (Strong electrophilic agent) attack liver tissues causing liver necrosis. -We can increase the level of GSH or overcome its depletion by; methionin (a precursor of GSH) & N-acetylcysteine (contains –SH). 7- Action on nucleic acids: E.g.: SO2 (air pollutant) + H2O HSO3(causing damage to DNA & mutation). E.g.: Benzidine Metabolism by HME N-hydroxybenzidine. Non-carcinogenic Mutagenic & Carcinogenic In cigarette smoke 8- Disruption of protein synthesis: Sometoxicants either increase or decrease protein synthesis leading to cellularinjury.
9-Lysosomal changes: a-Toxicants which causes labialization of lysosomal enzymes: E.g.: Hg , Cu , silica , nicotine , bee venom , hypervitaminosis A , monosodium ureate crystals deposited in gout increase lysosomal membrane permeability release of hydrolases cell death. b-Toxicants which causes stabilization of lysosomal enzymes: E.g.: Corticosteroids causes indirect toxicity by decreasing the response of the body defense mechanism .
Factors Influencing Toxicity There are many factors which can enhance, increase or decrease toxicity. These factors are divided into : I-Factors related to the host: A-The species. -Rats cannot vomit and expel toxicants before they cause severe irritation, whereas humans and dogs are capable of vomiting. Selective toxicity: refers to species differences in toxicity response between two species simultaneously exposed -an insecticide is lethal to insects but relatively nontoxic to mammals…??? malthion Oxidation by ME Hydrolysis (rapid in insects & slow in mammals) (slow in insects & rapid in mammals) Malaoxone Inactive substance (Lethal to insects)
B-Sex: -Male rats are 10 times more sensitive than females to liver damage from DDT &CCl4…? C-Age: -Some chemicals are more toxic to infants or the elderly than to adults. Example: 1)-Bounded bilirubin with p.p.+Sulfonamides replacement from P.P. binding sites. conjugated with glucoronyl transferase Free bilirubin excreted in adults (Low activity of GT + Immature B.B.B in neonates) Kernikterus (in newborn) 2)-Nitates(in well water) due to stomach pH is high in newborn Nitrite (oxidant) Oxidation Hb MetHb MetHb reductase (v.weak in newborns) Hypoxia
3)-Chloramphenicol conjugation by GT is low in neonates accumulation of it ,and it oxidizes Hb into MetHb Grey baby syndrome (hypoxia, cyanosis , collapse and death). D-Genetics: I-Pharmacogentices(Idiosyncratic reaction ): An odd response to a given normal dose of a drug on hereditary basis. 1) Succinylcholine apnea in individuals deficient in pseudo cholinesterase ….? 2) Individuals deficient in glucose-6-phosphate dehydrogenase suffer from hemolytic anemia upon using sulfa drugs , aspirin or naphthalene (oxidants) glucose-6-phosphate + NADP 2 GSH (protect RBCs from hemolysis by oxidants) G6PD GSH reductase 6-phosphogluconic acid + NADPH GSSG In case of G6PD deficiency NADPH GSH Oxidants attack RBCs hemolysis II-Toxicogentices: An odd response to a given toxicant on hereditary basis * smoking causes emphysema in certain individuals deficient in α1- antitrypsin. III-Hypersensitivity (allergic reactions): e.g. Some people suffer from an anaphylactic reaction when given penicillin.
Allergic reactions = an immune response that occurs after prior sensitization -These reactions range from mild, itchy ,severe skin rash to anaphylaxis -Intensity is determined by degree of sensitization and not by the dose. Penicillin as an example: We can get sensitization from molds in the air or from antibiotics given to animals we eat, we don’t necessarily have to be given a dose of Penicillin to become sensitized to it. Penicillin is not antigenic by itself because it is too small. To become capable of eliciting an allergic reaction, it must first be metabolized and then one of its metabolites attaches to endogenous protein to form a happen-protein complex. Now, antibodies can be made to this complex and an allergic reaction occur. E-Dietary factors 1) Calcium and proteins :increase GIT absorption of Pb 2)Low protein in diet:P.P. level decrease free drug toxicity . 3)Food containing tyramine as old cheese ,salted dried fish ,banana & wines increase MAOIs toxicity.
F-Health factors: 1)Acidosis: insulin activity decrease leading to hyperglycemia 2)Asthma: patient is more liable to the effect of air pollutants as SO2. 3)Kidney & liver diseases: toxicity of many drugs increase. End of factors related to Host
II-Factors releated to the poison: a-Dose It is the amount of a substance administered at one time. However, the number of doses, frequency, and total time of the exposure are also very important . Example: b-Routes of exposure -Ingested chemicals, when absorbed from the intestine, distribute first to the liver and may be immediately detoxified . -Inhaled toxicants immediately enter the general blood circulation and can distribute throughout the body prior to being detoxified by the liver. Intravenous › Inhalation › Interapertoneal › Intramuscular › Subcutaneous › Oral › Interadermal
c-Chemical structure -Silica (amorphous) after it is heated silica (crystalline) has little effect on health serious lung damage. -Cr3+ is relatively nontoxic whereas Cr6+ causes skin or nasal corrosion and lung cancer. d-Composition and formulation: ( mainly › absorption) -Concentration . -Lipid solubility. -Chemicals in liquid form are more toxic than those in solid form -Coloring agents as tartazin yellow cause allergy. -Micronization increase toxicity. -Vehicles as alcohols increase CNS depressant action of hypnotics. -Impurities; some herbicide as 2,4,5-trichlorophenoxy acetic acid may contain the toxic impurity DIOXIN which is mutagenic ,teratogenic and carcinogenic. -pH of the preparation (high acidity or alkalinity) cause local sever effect. -Low stability of the compound + bad storage condition increase toxicity as food contaminants aflatoxin ( it is a product of certain molds) e-The innate chemical activity : Some toxicants can quickly damage cells causing immediate cell death. Others slowly interfere only with a cell's function. -Hydrogen cyanide binds to cytochrome oxidase resulting in cellular hypoxia and rapid death -Nicotine binds to cholinergic receptors in the central nervous system (CNS) altering nerve conduction and inducing gradual onset of paralysis
III-Toxicokinetic factors: i-Factors affecting absorption: * GIT : Gastric content: -Empty stomach has higher emptying rate Toxicity. -Carbonated beverages increase G.E. Toxicity. -A full stomach with proteins & fats Toxicity. Secretion : Pepsin & HCl digest peptide poisons . GIT flora: migration of intestinal flora into the stomach in newborns due to their high gastric pH ,this flora can convert nitrates into nitrite, oxidizing Hb into metHb Hypoxia. *Skin (Thickness & Keratin layer protect the skin ): -Newborn (thin delicate skin). -Lipophilicity of insecticides. Toxicity -Cutting , abrasions & dryness of skin *Pulmonary: -Conc. Of toxicants in air. -Solubility of the toxin in blood & tissues. -Respiration rate. -Exposure time.
ii-Factors affecting metabolism (biotransformation): There are two types of metabolism :detoxification and bioactivation. Detoxification is the process by which a xenobiotic is converted to a less toxic form. Bioactivation is the process by which a xenobiotic may be converted to more reactive or toxic forms.
iii-Factors affecting distribution: Main mechanisms opposing distribution of the toxicants are: a-Plasma proteins: -Bilirubin in neonates???. -High affinity for binding to P.P. may cause toxicity due to drug interaction as sulfonamide displace tolbutamide from P.P. binding site causing hypoglycemia. b-Storage: -DDT is stored in fat tissues and upon short term diet ,mobilization of fats occur leading to release of DDT and toxicity. -Fluoride bind to calcium in bones flurosis. -Pb is stored in bones (non toxic to it) , osteoporosis mobilize Pb leading to toxicity. c-Special barriers (B.B.B.): -Mainly depends on lipid solubility
iv-Factors affecting excretion: -The kidney is the primary excretory organ, followed by the gastrointestinal tract, and the lungs (for gases). Xenobiotics may also be excreted in sweat, tears, and milk. • -Impaired cardiac , kidney or liver function causes slower elimination of toxicants and increases their toxic potential. • End of Toxicokintics factors • And Factors related to poison
IV-Chemical Interactions Humans are normally exposed to several chemicals at one time rather than to an individual chemical. Examples are:-Hospital patients on the average receive 6 drugs daily-Home influenza treatment consists of aspirin, antihistamines, and cough syrup taken simultaneously-Drinking water may contain small amounts of pesticides, heavy metals, solvents, and other organic chemical-Air often contains mixtures of hundreds of chemicals such as automobile exhaust and cigarette smoke-Gasoline vapor at service stations is a mixture of 40-50 chemicals -There are four basic types of interactions.
Additivity-A tranquilizer and alcohol, often cause depression equal to the sum of that caused by each drug.-Chlorinated insecticides and halogenated solvents (which are often used together in insecticide formulations) can produce liver toxicity with the interaction being additive. P.S. : this same combination of chemicals produces a different type of interaction on CNS. Chlorinated insecticides stimulate CNS whereas halogenated solvents cause its depression . So, the effect of simultaneous exposure on CNS is an antagonistic interaction. PotentiationIt occurs when a chemical that does not have a specific toxic effect makes another chemical more toxic. Example:-Warfarin (a widely used anticoagulant in cardiac disease) is bound to plasma albumin so that only 2% of the warfarin is active (FREE). Drugs which compete for binding sites on albumin increase the level of free warfarin to 4% causing fatal hemorrhage.
Antagonism It is often a desirable effect in toxicology and it is the basis for most antidotes. Examples include: Synergism -Exposure to both cigarette smoke and asbestos results in a significantly greater risk for lung cancer-The hepatotoxicity of a combination of ethanol and carbon tetrachloride is much greater than the sum of the hepatotoxicity of each. End of Factors affecting Toxicity
How do we measure toxicity? Toxicity is measured in numerous ways. The classic measure is ... LD50: Lethal Dose that kills 50% of the population. Dosage are measured in a mg toxin/kg body weight. While: Drug action is measured by: ED50: Effective Dose that produces the desired effect in 50% of the population. Dose-Response Curves characterize the response to different levels of a drug or toxin.
Dose Response curveThe dose-response correlates exposures and the spectrum of induced effects. -Generally, the higher the dose, the more severe the response. -The dose-response relationship is based on data from experimental animal, human clinical, or cell studies. -The dose-response curve normally takes the form of a sigmoid curve. For most effects, small doses are not toxic. -Threshold dose level :The point at which toxicity first appears ,and below which no effect occur. • -In the hypothetical curve above, no toxicity occurs at 10 mg whereas at 35 mg 100% of the individuals experience toxic effects. • -A threshold for toxic effects occurs at the point where the body's ability to detoxify a xenobiotic or repair toxic injury has been exceeded. For most organs there is a reserve capacity so that loss of some organ function does not cause decreased performance. For example, the development of cirrhosis in the liver may not result in a clinical effect until over 50% of the liver has been replaced by fibrous tissue.
-Knowledge of the shape and slope of the dose-response curve is extremely important in predicting the toxicity of a substance at specific dose levels. -Major differences among toxicants may exist not only in the point at which the threshold is reached but also in the percent of population responding per unit change in dose (i.e., the slope). -As illustrated above, Toxicant A has a higher threshold but a steeper slope than Toxicant B.
Response (ex. # of deaths or # of headaches) 50% Dose (ex. grams of carbon monoxide/ kg of body weight Dose-Response Curve A B
-Dose-response curves are also used to derive dose estimates of chemical substances: EDs & TDs. Toxic Doses (TDs) : the doses that cause adverse toxic effects. -The knowledge of the effective and toxic dose levels aides the toxicologist and clinician in determining the relative safety of pharmaceuticals. -As shown above, two dose-response curves are presented for the same drug, one for effectiveness and the other for toxicity. In this case, a dose that is 50-75% effective does not cause toxicity whereas a 90% effective dose may result in a small amount of toxicity.
The Therapeutic Index (TI) It is the ratio of the dose producing 50% toxicity to the dose needed to produce the 50% therapeutic response. - For example, if the LD50 is 200 and the ED50 is 20 mg, the TI would be 10 (200/20). A clinician would consider a drug safer if it had a TI of 10 than if it had a TI of 3. The use of the ED50 and LD50 doses to derive the TI may be misleading to safety, depending on the slope of the dose-response curves for therapeutic and lethal effects. To overcome this deficiency, toxicologists often use another term to determine the safety of a drug . The Margin of Safety (MOS). It is the ratio of the dose that is just within the lethal range (LD01) to the dose that is 99% effective (ED99). The MOS = LD01/ED99. -A physician must take care when prescribing a drug with MOS less than 1.
NOAEL and LOAEL:-No Observed Adversed Effect Level (NOAEL) -Lowest Observed Adverse Effect Level (LOAEL) -They are the actual data points from clinical or experimental animal studies. -They do not necessarily imply toxic or harmful effects ,and may be used to describe beneficial effects of chemicals as well.
Emergency Management of poisoning General approach for management of poisoned patient: 1-Emergency stabilization: provide the patient with good supportive care (maintain respiration & circulation). 2-Clinical evaluation: Identify the drug or poison as quickly as possible it include case history , physical exam and analytical procedures to analyze urine, blood, stomach contents (HPLC, mass spec. can be used) 3- Reduce or prevent absorption 4- Enhance the elimination of the poison. 5-Antidot 6-Supportive therapy and observation
Emergency stabilization: -ABCs, check gag reflex. -For patients with no obvious intoxication: obtain -IV access, draw electrolytes, obtain rapid fingerstick glucose, and send urine toxicology screen. -Consider ABG (if necessary to look for carbon monoxide, you must order this specifically). -Give isotonic fluid if hypertensive, but with caution (narcotics and naloxone can promote pulmonary edema). -If comatose with pinpoint pupils and decreased respirations, give 1-2 mg naloxone IV….???
A- Case history of poisoning:An accurate history include:i-Identification of the poison, amount and time of ingestion or length of contact (Empty bottles , If he was taken from garage….?,a factory…etc).ii-The patient's psychological profile: This is difficult because the poisoned individual may be unconscious, unresponsive or confused. Information usually obtained from relatives or friends.iii-Identify if the patient performed any self treatment or took any medication? B-Physical examination: Some poisons produce clinical characteristics which strongly suggest the type of the poison 1-Presence of characteristic odour; phenol, alcohol, kerosene, bitter almond odour of cyanide 2-Skin manifestation: a- Changes in the skin Color - Red in carbon monoxide poisoning. - Flushed and dry in atropine poisoning. - Flushed and sweaty in LSD and cocaine. - Cyanosed in cyanide, nitrites and carbon monoxide. • -Yellow “Jaundice” in acetaminophen, carbon tetrachloride b- Needle markers: Indicate addiction by intravenous route e.g. heroin and cocaine. c- Alopecia: in Thallium. d-Burns & corrosion: Acids & alkali
3-Eye manifestation: a- Eye globe: i- Lacrimation: In organic phosphorous ii- Nystagmus: In barbiturates. b- Pupils: i- Dilated reactive pupils: In alcohol and cocaine. ii- Dilated fixed pupils: In atropine. iii- Constricted pupils: In phenol and opium. 4-Gastro-intestinal manifestations: a- Mouth: i- Salivation: In organophosphorous compounds. ii- Dry mouth: In atropine and other anticholinergic drugs. iii- Corrosion : With corrosives. iv- Gum discoloration: Lead causes blue line. Cadmium causes yellow line. Mercury causes grey line. b- Vomiting: Most poisons except narcotics. c- Abdominal: i- Diarrhea in all heavy metals except lead. ii- Constipation with opium and lead.
5-Cardio-vascular manifestations: a- Tachycardia: In alcohol, atropine. b- Bradycardia : In digitalis ,opium, cyanide & β blockers. c- Rise in blood pressure: Lead,amphetamine, and tricyclic antidepressant. d- Hypotension: In barbiturates. 6-Respiratory manifestations: -Acute respiratory failure in barbiturates. -Pulmonary edema due to inhalation of petroleum and arsenic fumes. 7-Central nervous system manifestation: a- Coma: Barbiturates, Paraldehyde, and ethylene glycol. b-Convulsions: Amphetamines, camphor, chlorinated hydrocarbons, lead, strychnine, cocaine, alcohol, anticholinergic, antihistaminic. c-Hyperpyrexia: Salicylates, amphetamine and theophyline. d-Hypothermia: Clonidine and tricyclic antidepressants. e-Muscle fasciculations: With nicotine, strychnine and camphor. f-Tremors: Occurs with amphetamines, carbon monoxide, hallucinogenic drugs, xanthines (theophylline) and tricyclic antidepressants.
C- Analytical toxicological laboratory screening: These give the correct diagnosis and could be done on biological fluids .This usually include: -CBC -Serum electrolyte level. -BUN -Blood glucose, …… ,prothrombin time. -Urine analysis. -X-ray on the chest. -Spinal tap (meningitis (coma, fever) Once emergency procedures have been performed and the poisoned patient is stabilized, or at least is out of immediate danger, additional steps can be taken to remove the poison, prevent a delay absorption, enhance excretion, or administer a specific antidote.
III-Prevent absorption and removal of poison A general rule is that nothing should be administered orally to an unconscious patient A)- Topical decontamination 1- Skin decontamination: Rapid decontamination is needed specially if the poison is a corrosive or is easily absorbed from the skin. - Wash contaminated areas as well as exposed areas with warm water or saline , with careful washing of the skin, behind ears, under nails, and skin folds. Phenol: Can apply olive oil . Oxalic acid: Soak the affected area with solution of calcium gluconate. Organophosphorus: Soap water 2-Eye decontamination: i- Irrigation of the eyes with large amounts of water. ii- The eye is usually affected by a corrosive :apply anesthetic drops e.g. cocaine HCI (Xylocaine) After first aid treatment the patient should be referred to an ophthalmologist in order to asses and treat any inflammation. 3- Demulcents Many plants and chemicals cause oral and gastric mucosa irritation but no serious toxicity. Management for these acute ingestion may include ice cream or milk. Egg whites, which serve as a source of readily available protein, have been given for corrosive intoxications.
B)-If the poison was ingested: 1- Dilution: By using water & milk immediately after poisoning. - This reduce the gastric irritation induced by many ingested poisons. 2- Milk provides dilution and is also a demulcent. 2- Delay gastric emptying: a)-Emesis : induced by i-Syrup of Ipecac: orally administered ii- Apomorphine: given by s.c. injection (most rapid) ,but cause CNS depression iii- Liquid detergent 30-45 ml in 120-240 ml juice or water. Contraindications: 1- Ingestion of a strong acids ,alkalis or hydrocarbon e.g. kerosene???????? 2-Do not induce vomiting if the patient: • Is Unconscious or comatose, convulsant , has sever cardiovascular disease or, emphysema or under 6 months of age?? b)-Gastric lavage: Gastric lavage is only effective when ingestion of the poison is discovered within 4 hours except salicytates may be within 10 hours (it sticks to the mucous membrane).This procedure is often reserved for patients with impaired consciousness and uncooperative or when ipecac failed to produce emesis. Solutions used :sodium bicarbonate, saline, tannic acid or water. Contraindications: Strong acid and alkalis, in convulsion, in sever respiratory and cardiac insufficiency???
3-Adsorbents : activated charcoal, starch and flour . Activated charcoal: is administered orally to adsorb or bind toxins and allows them to pass from the GIT without being absorbed into the systemic circulation. Contraindications: 1- Absence of the bowel sounds . 2- Intestinal obstruction. 3- Many preparation add sorbitol to the mixture ,so repeated dose lead to diarrhea, dehydration, hypernatraemia in children and elderly. 4-DO NOT give with syrup of ipecac because it will bind the syrup of ipecac. 4-Cathartic Agents: Such as Magnesium citrate, sodium sulfate , polyethylene glycol and sorbito1. Careful monitoring of the fluid and electrolyte status is necessary. Contraindications: -Catharsis should not be attempted when the poison is strongly corrosive, the patient has electrolyte disturbance or bowel sounds are absent. -Magnesium containing cathartics-should not be used in cases of renal failure…… because of the possibility of causing CNS depression due to accumulation of high concentration of magnesium in the serum. -Sodium containing cathartics are, likewise, best avoided by persons with congestive heart failure -Oil cathartics e.g. castor oil may increase the absorption of fat-soluble poisons such as pesticides.
IV-Enhancement of Excretion 1-Forced Diuresis: its useful to enhance renal elimination of poisons. Saline to expand fluid volume and furosemide may be used to enhance diuresis. 2-Acid Diuresis: with ammonium chloride can enhance the elimination of weak bases e.g. phencyclidine, amphetamine, strychnine and quinidine. 3-Alkaline Diuresis: with Sodium bicarbonate can remove weak acids (e.g. salicylates and Phenobarbital). 4-Dialysis and Hemoperfusion -As adjuncts for management of severely intoxicated patients. -Dialysis and hemoperfusion should never replace more specific antidotes. -These procedures would be of little value in treating acute ingestions of cytotoxic poisons such as cyanide which produce toxic effects very rapidly.
V- Specific Antidote Chemical antidotes: In oxalic acid poisoning, absorption produces renal damage. Calcium salts react with oxalic acid to yield a poorly soluble compound, calcium oxalate, which passes through the intestine without being absorbed. Antidotes such as dimercaprol (BAL) and deferoxamine form chemical chelates with heavy metals. Chelated complexes are water soluble and readily excreted by the kidney. Receptor antidotes: Compete with the poison for receptor sites. -Naloxone reversal of morphine-induced respiratory depression -Cholinergic blockade by atropine (parathion poisoning). -For atropin or other anticholinergic poisons, physostigmine is a specific antidote. Dispositional antagonism: In acetaminophen overdose, a toxic metabolite is conjugated with glutathione(a sufhydryl ( sH group donor). When glutathione reserves are depleted……..hepatotoxicity. N-acetylcysteine is also a source of sulfhydryl groups which serve the same function as endogenous glutathione. Acetaminophen and its toxic metabolite are therefore detoxified and the liver cells are not subjected to prolonged toxicity. Function (physiologic) antagonist: Epinephrine reverses the bronchoconstriction due to anaphylactic reaction following administration of certain drugs.