Download
1 / 48
490 likes | 738 Views
Hematopoietic Stem Cell Transplant (HCT) for Nonmalignant Disorders Evan Shereck, M.D. September 13, 2013. Objectives. Overview of nonmalignant disorders - Immunodeficiencies - Genetic/metabolic disorders - Inherited blood disorders - Bone marrow failure syndromes

E N D
Hematopoietic Stem Cell Transplant (HCT) for Nonmalignant Disorders Evan Shereck, M.D. September 13, 2013
Objectives • Overview of nonmalignant disorders - Immunodeficiencies - Genetic/metabolic disorders - Inherited blood disorders - Bone marrow failure syndromes • Review outcome of HCT for selected nonmalignant diseases • Discuss donor issues specific to nonmalignant diseases
Indications for HCT for Patients < 20 years 800 Allogeneic (Total N=1,496) 700 Autologous (Total N=880) 600 500 Number of Transplants Number of Transplants 400 36% 300 200 100 0 Other ALL AML Aplastic HD NHL MDS/MPD CML Other Non- Cancer Anemia Leuk Malig Disease
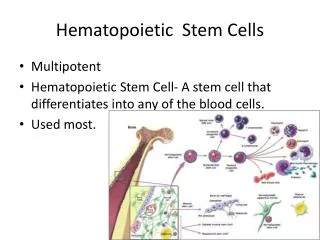
Primary Immunodeficiencies • Genetically heterogeneous group of diseases affecting distinct components of innate and adaptive immunity - Lymphocytes (T, B cells) - Natural killer cells - Neutrophils - Dendritic cells - Complement proteins • More than 120 gene defects have been described
Natural History of Inherited Immunodeficiencies • Spectrum of disease depends on genetic defect
Outcomes of HCT for SCID MRD (matched related donor), Haplo (haplocompatible family donor), MUD (matched unrelated donor) Percentage indicates overall survival , Number in parentesis = number of patients
Effect of Age on Transplant Percent Surviving Day of Life at Transplant Rebecca H. Buckley, J. All & Clin Immunol, 2012
Unique Features for HCT for SCID • Bad disease need HCT ASAP, any suitable donor • Conditioning not needed for “complete” SCID • Most patients needs some form of conditioning - Maternal T-cell engraftment at birth - Dysfunctional/over-reactive T-cells • High rates of toxicity, TRM and GVHD observed • Goal is to condition with minimal amount of conditioning necessary to achieve engraftment • Full donor chimerism usually not necessary • Newborn screening in some states
Inherited Metabolic Diseases • Genetic defects in enzymes accumulation of metabolic products in body organs progressive dysfunction death • Multiple diseases, some amenable to HCT some not Rule of thumb: If replacing leukocytes can generate the missing enzyme, then HCT may be effective • Time is of essence Ultimate outcome and QOL not improved if end-organ symptoms are present
Metabolic Disorders & Transplantation Standard of care Under Investigation Hunter I-cell Recessive Osteopetrosis Niemann-Pick Gaucher Farber Tay-Sachs • MPS IH (Hurler) • Metachromatic leukodystrophy (MLD) • Globoid Cell leukodystrophy (Krabbe) • -mannosidosis • acid lipase deficiency (Wolman disease) • Cerebral ALD
Strategies to Replace Enzymes Enzyme replacement therapy (“ERT”) • Required for the life of the patient • Does not penetrate into the brain Gene Therapy • Correction of patient’s own cells • Over-produce missing enzyme in other cells Cellular therapy with “normal” cells • HCT: how does this help the brain?
The Challenge of Fixing the CNS: Microglia • Cells of the immune system within the brain • About 15% of cells in the brain are microglia • Derived from hematopoietic precursors • Likely takes months for these cells to make their way into the brain • Timing is of essence
Hurler Syndrome (MPS IH) Signs and symptoms Macrosomia Developmental delay Chronic rhinitis/otitis Corneal clouding Obstructive airway disease Hearing loss Umbilical/inguinal hernia Enlarged tongue Cardiovascular disease Skeletal deformities Hepatosplenomegaly Carpal tunnel syndrome Joint stiffness Neufeld EF, Muenzer J. In: Scriver C, Beaudet A, Sly W, Valle D, eds. The Metabolic and Molecular Bases of Inherited Disease. New York, NY: McGraw-Hill; 2001:3421-3452.
HCT for Hurler syndrome • Since early 1980s, > 500 transplants done • Considered the standard of care for Hurler • Donor-derived microglia engraft over 4-6 months, providing enzyme to the CNS • Enzyme infusions used for less severely effected patients (Scheie), as those without severe neurologic deterioration • Opportunity exists for combination therapy
Event-Free Survival Post HCT for Hurler’s Boelens JJ et al, Pediatr Clin of N. Am, 2010
Neuro Outcomes for Hurler’s The sooner the better! Mental = chronological age in 64% transplanted before age 2 Vs. Mental = chronological age in < 25% transplanted after age 2 P=0.01 Peters: Blood 1998: 91 (7) 2601-08
Unique Features for HCT for Metabolic Disorders • High risk for toxicity and mortality • High risk for rejection/ graft failure • Must balance these risks to achieve best outcomes • Full chimerism not needed to achieve clinical effect • Reduced-intensity regimens preferred in most patients • Related donors carriers of enzyme defect are not good donors. Unrelated cord blood preferred • Hard to measure effect of transplant on CNS manifestations • Many of the somatic symptoms do not improve after BMT, some may ‘worsen’ • Lack of data a big problem for insurance companies
Limitations of HCT for Rare Metabolic Disorders • Magic in numbers… • Rare nature of diseases and variation in severity limits the power of studies, ability to randomize, etc. • Well designed cooperative trials important, but limited resources, experience complicates assessments and outcome analysis • Growing interest in newborn screening may provide a chance to treat very early in the course of disease; cooperative trials may be important
HCT for Hemoglobinopathies • Sickle cell disease • Thalassemia major
Sickle cell disease World’s most common serious disease due to a single gene mutation Normal …..G A G G A G….. Sickle (6glu val) …..G T G G A G…..
Inheritance of Sickle Cell Disease • Autosomal recessive inheritance 2 parents with HgB S trait: 25% risk of child with SCD Not just in African Americans • African ancestry • Caribbean, Central/South America • Mediterranean (Greece, Italy) • Middle East • India
Sickling of Red Blood Cells • VASO-OCCLUSION • ANEMIA • HEMOLYSIS CLINICAL MANIFESTATIONS: Acute: - Painful crisis - Acute chest syndrome - Stroke - Splenic sequestration - Aplastic crisis - Priapism Chronic organ dysfunctions: - Spleen - Kidneys - Lungs: Pulmonary hypertension - Osteonecrosis - Eyes - Skin ulcers - Liver
Therapeutic Approaches for Sickle Cell Disease • Hydroxyurea (increase % fetal Hgb, decrease sickling) • Symptomatic management • Exchange transfusions and iron chelation therapy • Some patients may benefit from HCT - Recurrent pain crisis - Recurrent acute chest syndrome - CNS disease • Benefit of HCT decreases as age increases
Thalassemia Major • Inability to produce adequate amount of hemoglobin • Autosomal recessive inheritance • > African, Mediterranean, Asian descent • Chronic hemolytic anemia, poor growth, infections, bone deformities • Death, if untreated
Management of Thalassemia Major • Symptomatic management • Chronic transfusions and iron chelation therapy + splenectomy • Only known cure is HCT • Goal is to offer HCT early before chronic iron deposition causes end-organ damage
Matched Sibling HCT for Sickle Cell 93% 85% 9% Time (years) after BMT
Unrelated Donor HCT for Thalassemia Kaplan-Meier probabilities of survival, thalassemia-free survival, nonrejection mortality, and rejections for 32 thalassemia patients who received transplants from HLA-matched unrelated donors (parenthesis: 95% confidence limits at 2 years). La Nasa G et al. Blood 2002;99:4350-4356
Survival for Unrelated Cord Blood Transplantation for Hemoglobinopathies Sickle cell Thalassemia Ruggeri A, Eurocord, 2011
Unique Features of HCT for Hemoglobinopathies • High risk of rejection - Myeloablative conditioning is preferred • Many patients with end-organ damage cannot tolerate full conditioning reduced intensity • Carrier relatives (HgB S trait) can be donors • Very small matched unrelated donor pool available Unrelated cord blood attractive, but risk of rejection high • Benefit of HCT decreases as age increases
Severe Aplastic Anemia (SAA) • Two of the following: • Neutrophils < 500/L (1500-5000) • Platelet count < 20 x 109/L (180-440) • Abs. reticulocyte count < 40 x 109/L (20-80) AND • Bone marrow biopsy < 25% cellularity Carmitta et al, Blood, 1976
Causes of Aplastic Anemia Inherited Acquired Pregnancy Drugs Infections Immune disorders Benzene Ionizing radiation Idiopathic • Fanconi anemia • Dyskeratosis congenita • Diamond Blackfan anemia • Shwachman-Diamond syndrome
Aplastic Anemia- Treatment • Supportive care • Immunosuppressive therapy • HCT
Probability of Overall Survival Kennedy-Nasser et al, Biol Blood Mar Transpl, 2006
Unique Features of Aplastic Anemia • May be able to use reduced conditioning • Related and Unrelated have similar outcomes • Try to transplant early • May need prolonged immunosuppression taper
Conclusions • Increasing use of HCT for non-malignant disorders • Donor/conditioning different depending on dz • Early consultation to HCT team for non-malignant dz
Thank You! Nycole Ferguson Shirley Mason Christina Burgin Julian Kern Meena Mishra Amanda Tuggle The Doernbecher Pediatric BMT Team • Eneida Nemecek, MD, MS • Bill Chang, MD, PhD • Peter Kurre, MD • Allison Franco, RN, BSN, CPHON • Erica Soler, RN, PNP All the patients and families whose care we have been privileged to provide