Download
1 / 43
430 likes | 445 Views
Explore the impact of accurate medication profiles on patient safety under California's SB1254 law. Learn from a multicenter quality improvement study and strategies for implementation.

E N D
SB 1254: MEDICATION PROFILES FOR HIGH RISK PATIENTS Multicenter California Quality Improvement Project August 1, 2019
Webinar Objectives • Review the literature related to errors and potential harm associated with inaccurate medication histories • Review SB1254 implementation strategies • Describe the rationale for the multicenter quality improvement (QI) study on the impact of SB1254 • Review elements of the QI study including design, responsibilities of participating sites and tools • Provide an opportunity for Q and A
Project Investigators Rita Shane, PharmD, FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Donna Leang, PharmD, MHDS, BCPS, FCSHP Medication Safety Manager Cedars-Sinai Medical Center • Sarah Stephens, PharmD, BCPS, CPPS Medication Safety Coordinator Kaweah Delta Health Care District Sarah A. Bajorek, PharmD, BCACP Pharmacy Supervisor Transitions of Care UC Davis Health Naira Barsegyan, PharmD Program Coordinator Cedars-Sinai Medical Center Ryan Hays, PharmD PGY-2 Pharmacy Administration Resident Cedars-Sinai Medical Center
Background • The 2019 Joint Commission Hospital National Patient Safety Goal NPSG.03.06.01 aims to improve the safety of using medications • This goal acknowledges the challenges with medication reconciliation as well as the evidence that medication discrepancies can negatively affect patient outcomes • This program will educate participants about the importance of pharmacy management of medication histories upon admission and introduce a multicenter study to report the impact of Senate Bill 1254 on patient safety
Senate Bill 1254 – Medication Histories for High-Risk Patients • Passed into Law September 22, 2018 • Law enforced beginning January 1, 2019 Hospital Pharmacies: medication profiles or lists for high-risk patients The bill requires hospital pharmacy staff to obtain an accurate medication profile or list for each high-risk patient upon admission as part of California State Board of Pharmacy Law.
Literature on Errors Associated with Inaccurate Medication Histories
Sources of Medication Lists • Errors introduced in any of these settings can become “hardwired” • into the electronic health or paper record • ED/Hospital • Nurses • Physicians • Pharmacists • Pharmacy technicians • Pharmacy residents, students • Outpatient Settings • Certified medical assistants • Physicians • Community pharmacies • Patients • Skilled Nursing Facility • Nurses • Physicians • Home • Patients • Family members • Caregivers • Home Health nurses
Evidence Summary Problem • 20% of admissions are medication-related1 • High risk patients have 8 errors on admission medication lists2 • Only 5.3% of patients 65 year or older on >5 medications have accurate lists3 • One third of inpatient orders have errors and 85% originate from the medication history4 • Up to 70% of patients have errors on their medication list when admitted and up to 59% of errors can cause harm5 • Up to 80% of patients have at least 1 medication error at discharge6 Davies EC, et al. Br J Clin Pharmacol. 2010 Nov;70(5):749-55. Pevnick JM, et al. BMJ Quality and Safety. 2018;27(7):512-520. Kaboli PJ, et al. Am J Manag Care. 2004 Nov;10(11 Pt 2):872-7. Gleason KM, et al. J Gen Intern Med 2010;25:441–7. Tam VC, et al. Canadian Medical Association Journal. 2005; 173(5):510-5. Kilcup M, et al. J Am Pharm Assoc. 2013;53(1):78-84.
Evidence Summary (con’t) Solution • On admission, studies demonstrate increased accuracy of medication lists obtained by pharmacy staff vs. usual care • Accuracy rates: • Nurses, 20%; Hospitalists, 50%; Technicians, 100%7 • Nurses 14% vs pharmacy technicians 94% (p<0.0001)8 • At discharge, pharmacists identified errors in medication lists in 49% of patients and problems in an additional 16% vs. usual care9 Gardella JE, et al. Joint Commission J Qual Safety. 2012, 38(10):45288. Markovic M, et al. P T. 2017;42(1):41-46. Schnipper JL, et al. Arch Intern Med, 2006; (166):565-71.
Evidence Summary (con’t) Business Case Cost of Harm Benefits • Cost of adverse drug event (ADE): $2,262- $5,7907,10-13 • Increased length of stay due to ADE: 3.1 days13 • Cost/readmission ~$12,300-13,80014 • 75% reduction in ADEs7 • 41 minutes of nursing time saved/patient16 • Cost-effective to utilize technicians for medication histories; $830,0007 • Patients have an accurate medication list upon discharge • Reduced readmissions • Enables clinicians to practice at the highest level of their license and training Gardella JE, et al. Joint Commission J Qual Safety. 2012, 38(10):45288 Classen D, et al. JAMA, 1997; 22-29;277(4):301-6. Bates DW, et al. JAMA, 1997;22-29;277(4):307-11. Hug BL, et al. Jt Comm J Qual Patient Saf., 2012;38(3):120-6. https://psnet.ahrq.gov/resources/resource/24087 Accessed 9/23/17 https://www.speechmed.com/cost-hospital-readmission/ Accessed 9/25/17 Hennen CR, et al. Am J pharm benefits, 2014;6(2):71-75. Feldman LS, et al. Journal of Hospital Medicine, 2012; 7(5): 396-401.
Sarah A. Bajorek, PharmD, BCACP Pharmacy Supervisor – Medication Reconciliation and Transitions of Care UC Davis – implementing MARQUIS 2 best practices
UC Davis Demographics • 627-bed academic medical center • Level 1 trauma center • Magnet recognized • Nationally ranked in 11 specialties by U.S. News & World Report (2017-2018) • MARQUIS 2 site
MARQUIS 2 • Multi-center Medication Reconciliation Quality Improvement Study (MARQUIS) • Mentored implementation of evidence-based medication reconciliation best practices identified via MARQUIS 1 • Evaluate the effect of MARQUIS 2 program on unintentional medication discrepancies
MARQUIS Intervention Components • Medication Reconciliation Bundle • “Best Possible Medication History” • Reconciliation at discharge • Patient counseling • Forwarding information to next provider • Risk Assessment • Intense vs. Standard Bundle depending on patient risk • Training providers in taking a BPMH and in performing discharge counseling • Improving access to preadmission medication sources • Encouraging patient-owned medication lists • Facilitating access to other medication sources (e.g., pharmacies) • Other high-risk, high-reward interventions • Implementing and improving HIT • Utilizing social marketing • Engaging community resources
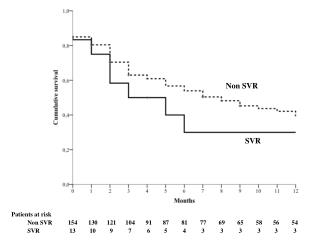
MARQUIS Results • Baseline – average 5 clinically significant discrepancies per patient • Intervention patients • Less than 1 clinically significant discrepancy per patient • 64% relative reduction in discrepancies compared to control • 89% accuracy in medication list compared to 52% for control
Lessons Learned – Engaging Providers and Staff • Structured quality improvement • Meet with stakeholders in small settings to understand barriers and obtain support • Build in accountability by defining roles and responsibilities • Ongoing education on best practices • Use data to your advantage
Sarah Stephens, PharmD, CPPS, BCPS Medication Safety Coordinator Kaweah Delta’s experience with SB1254
Kaweah Delta Demographics • 581-bed academic regional medical center (400 acute care beds) • Level 3 trauma center • Serving over 454,000 in Tulare County
Clinical Model *High risk medications = anticoagulants, insulin, digoxin, narcotics, antiplatelet agents, transplant medication, home chemotherapy agents
Multicenter California Quality Improvement (QI) Project Demonstrating Impact of SB 1254
Study Objectives • Determine the number of drug-related problems (DRPs)^ prevented and the associated potential harm as a result of SB 1254 • Determine the cost savings associated with preventing harm ^Drug-related problems (DRPs): inaccuracies (including errors) identified on the medication list that may lead to errors in inpatient and discharge orders or adverse drug events
Outcomes • Number of DRPs identified, total number and mean per patient • Percent of patients with at least 1 DRP • Type and severity of DRPs • Projected total costs avoided by preventing harmful medication errors due to inaccurate medication histories
Study Design • Participating institutions to capture DRPs avoided for 6 weeks (Jan to Mar 2020) • Standardized categories of errors intercepted (e.g. wrong dose, wrong frequency, etc.) • Standardized methodology to rate level of harm prevented by intercepting errors (NCC MERP^) • Standardized documentation process of errors intercepted (data collection sheet/form) • Inter-rater methodology ^NCC MERP: National Coordinating Council for Medication Error Reporting and Prevention
Potential Error Types • Allergy • History of ADR • Drug-Disease Interaction • Drug-Drug Interaction • Drug-Lab Interaction • Duplicate Therapy • Incomplete Order • Therapy Omission • Wrong Concentration • Wrong Dose/Rate/Frequency • Wrong Duration • Wrong Medication Ordered • Wrong Route/Dosage Form • Wrong Timing • Wrong Patient • Not Indicated
Adaptation of the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP)
Cedars-Sinai Medical Center Potential Error Severity Adapted from NCC MERP* Low Capacity for Harm Category A: Circumstances or events that have the capacity to cause error Category B: An error could have occurred but the error would not reach the patient (An "error of omission" does reach the patient) Category C: An error could have reached the patient but would not cause patient harm Serious Category D: The identified and intercepted error could have reached the patient and would have required monitoring to confirm that it resulted in no harm to the patient and/or required intervention to preclude harm Category E: The identified and intercepted error may have contributed to or resulted in temporary harm to the patient and required intervention Category F: The identified and intercepted error may have contributed to or resulted in temporary harm to the patient and required initial or prolonged hospitalization Life Threatening Category G: The identified and intercepted error may have contributed to or resulted in permanent patient harm Category H: The identified and intercepted error may have required intervention necessary to sustain life Category I: The identified and intercepted error may have contributed to or resulted in the patient’s death *Pharmacists determine the potential severity of the outcome had the error not been intercepted
Responsibilities for Participants Establish a medication history program Establish an error documentation system to capture DRPs Participate in conference calls and in-person meeting (e.g. Seminar) IRB Enrollment (quality improvement exemption) Oversight of data collection (lead from each site) Identify and engage medical staff to validate potential harm prevented Individual site data analysis Submit aggregate results
Tools for Participating Sites • List of primary investigators and contact information • Study background, objectives, methods, timeline, etc. • Definitions of error types (e.g. wrong dose, wrong frequency, etc.) • Definitions of level of harm avoided (NCC MERP) • Data collection form for organizations that want to collect data via paper form • Data collection Excel spreadsheet for organizations that will collect data manually • Therapeutic class reference list • Aggregate data elements (minimum required for study participation) • IRB quality improvement exemption template • Examples of error documentation systems/processes
Special Thank You • Senator Jeff Stone, PharmD and his office, special thanks to Brittny Garcin • CHA Medication Safety Committee • Daniel Kudo, PharmD, FCSHP, APh, Associate Professor, Keck Graduate Institute • Joseph Sky, MD, FACC Lt Col, Chief of Cardiology, David Grant Medical Center, United States Air Force, Travis Air Force Base • Hattie Hanley, MPP, Right Care Project Director • Mithu Molla, MD, MBA, Section Chief for Hospital Medicine at UC Davis Health • Joshua Pevnick, MD, Associate Director, Division of Informatics, Cedars-Sinai Medical Center • BJ Bartleson, RN, MS, NEA-BC, Vice President, Nursing & Clinical Services, California Hospital Association • Cedars-Sinai Medical Center • CSHP
References • Davies EC, Green CF, Mottram DR, et al. Emergency re-admissions to hospital due to adverse drug reactions within 1 year of the index admission. Br J Clin Pharmacol. 2010 Nov;70(5):749-55. • Pevnick J.M., Jackevicius C.A., Palmer K.A., Shane R, et al. Improving admission medication reconciliation with pharmacists or pharmacy technicians in the emergency department: a randomized controlled trial. BMJ Quality and Safety. 2017; DOI: 10.1136/bmjqs-2017-006761 • Kaboli PJ, McClimon BJ, Hoth AB et al. Assessing the accuracy of computerized medication histories. Am J Manag Care. 2004 Nov;10(11 Pt 2):872-7. • Gleason KM, McDaniel MR, FeinglassJ, et al. Results of the medications at transitions and clinical handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med 2010;25:441–7. • Tam VC, Knowles SR, Cornish PL, et al. Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. Canadian Medical Association Journal. 2005; 173(5):510-5. • Kilcup M, Schultz D, Carlson J, Wilson B. Post discharge pharmacist medication reconciliation: Impact on readmission rates and financial savings. J Am Pharm Assoc. 2013;53(1):78-84. • Gardella JE, Cardwell TB, Nnadi M, Improving medication safety with accurate preadmission medication lists and postdischarge education, Joint Commission J Qual Safety. 2012, 38(10):45288 and http://www.todayshospitalist.com/making-the-business-case-for-med-rec/ Accessed 9/20/17 • Markovic M, Mathis AS, Ghin HL, Gardiner M, . A comparison of medication histories obtained by a pharmacy technician versus nurses in the emergency department. P T. 2017;42(1):41-46. • Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med, 2006; (166):565-71. • Classen DC, Pestotnik SL, Evans RS, Lloyd JF, Burke JP. Adverse drug events in hospitalized patients. Excess length of stay, extra costs, and attributable mortality. JAMA, 1997; 22-29;277(4):301-6. • Bates DW, Spell N, Cullen DJ, Burdick E, Laird N, Petersen LA, Small SD, Sweitzer BJ, Leape LL. The costs of adverse drug events in hospitalized patients. Adverse Drug Events Prevention Study Group. JAMA, 1997;22-29;277(4):307-11. • Hug BL, Keohane C, Seger DL, Yoon C, Bates DW. The costs of adverse drug events in community hospitals. Jt Comm J Qual Patient Saf., 2012;38(3):120-6. • https://psnet.ahrq.gov/resources/resource/24087 Accessed 9/23/17 • https://www.speechmed.com/cost-hospital-readmission/ Accessed 9/25/17 • Hennen CR, Jorgenson JA. Importance of medication reconciliation in the continuum of care. Am J pharm benefits, 2014;6(2):71-75. • Feldman LS, Costa LL, Feroli ER, Nelson T, Poe SS, Frick KD, Efird LE, Miller RG. Nurse-pharmacist collaboration on medication reconciliation prevents potential harm. Journal of Hospital Medicine, 2012; 7(5): 396-401.
Project Investigator - Biography Rita Shane, PharmD, FASHP, FCSHP is the Chief Pharmacy Officer and Professor of Medicine at Cedars-Sinai Medical Center, an 886-bed acute, tertiary care, teaching institution in Los Angeles and Assistant Dean, Clinical Pharmacy Services, at the University of California, San Francisco, School of Pharmacy. She is responsible for over 350 staff members. Dr. Shane’s research and legislative efforts led to tech check tech in California and Senate Bill 1254requiring high-risk patients to have medication lists obtained by pharmacy staff. She has published 100 papers and given over 200 presentations nationally and internationally.
Project Investigator - Biography • Donna Leang, PharmD, MHDS, BCPS, FCSHP is the Medication Safety/Transitions of Care Program Manager at Cedars-Sinai Medical Center. She graduated from and completed her PGY-1 Pharmacy Practice residency at the University of California, San Francisco. She completed her PGY-2 Pharmacy Administrative Residency at Cedars-Sinai and in 19 years, has led very roles including Med/Surg Supervisor, Compliance, and Medication Safety. Dr. Leang has lead the CSMC TOC program since November 2014 and under the guidance of the CPO, has increased TOC staffing by sixty percent. Donna led the CSMC CSHP Transitions of Care Certificate program that was offered through CSHP between 2017-2019, training over 100 pharmacy staff.
Project Investigator - Biography Sarah Stephens, PharmD, BCPS, CPPS is the Medication Safety Coordinator for Kaweah Delta Health Care District in Visalia, California. The majority of Dr. Stephens’ career has focused in acute care adult internal medicine. Current initiatives and research interests include reducing medication errors in the areas of anticoagulation and pain management, improving transitions of care with an emphasis on discharge medication reconciliation, and evaluating safety culture. Dr. Stephens is a member of the California Hospital Association Medication Safety Committee and is a Director-at-Large for ASHP’s Section of Inpatient Care Practitioners.
Project Investigator - Biography Sarah A. Bajorek, PharmD, BCACP, is the Pharmacy Supervisor for Transitions of Care and Medication Reconciliation at UC Davis Health and an Assistant Clinical Professor with UC San Francisco’s School of Pharmacy. At UC Davis, she leads the Transitions of Care and Medication Reconciliation team, which consists of pharmacy technicians and pharmacists completing best possible medication histories (BPMH) and medication reconciliation for high risk patients.
Project Investigator - Biography Naira Barsegyan, PharmD, is a Program Coordinator at Cedars-Sinai Medical Center. She graduated from Loma Linda University and completed a general acute care residency at Adventist Health – Glendale. Afterwards, she went on to complete a PGY2 in Health System Pharmacy Administration at Cedars-Sinai Medical Center. Her professional interests include pharmacy regulatory compliance, medication safety, and teaching.
Project Investigator - Biography Ryan Hays, PharmD, is the PGY-2 Health System Pharmacy Administration and Leadership resident at Cedars-Sinai Medical Center. He is a graduate of the University of Southern California and completed a PGY-1 Pharmacy Residency at Cedars-Sinai Medical Center. His interests include medication safety, drug information, and pharmacy informatics.