Download
1 / 63
630 likes | 1.02k Views
Behaviour Disorders in Adolescents: Clinical and Psychopathological Assessment. Mª.C. Ballesteros (Hospital Clínico Universitario de Valladolid) J.L. Pedreira (Hospital Infantil Universitario Niño Jesús, Madrid).

E N D
Behaviour Disorders in Adolescents: Clinical and Psychopathological Assessment Mª.C. Ballesteros (Hospital Clínico Universitario de Valladolid) J.L. Pedreira (Hospital Infantil Universitario Niño Jesús, Madrid)
Behaviour Disorders and International Systems of Mental Disorders Classification/1 • DSM-III (1980): Basic conditions are sociabilization: • Undersocialized, aggressive or not aggressive • Socialized, aggressive or not aggressive • DSM-III-R (1987): Basic conditions are individual or grupal behaviour disorder or aggressiveness
Behaviour Disorders and International Systems of Mental Disorders Classification/2 • DSM-IV (1994): Basic conditions are disocial behaviour and age: • Aggression on people and animals • Destruction of property • Deceitfulness or theft and serious violations rules • ICD-10 (1992-94): Basic condition is context of disocial disorder: • Disocial disorder only on family context • Disocial disorder undersocialized children • Disocial disorder socialized children • Oppositional defiant disocial disorder
HOLLISTIC AND COMPREHENSIVE CLINICAL ASSESSMENT IN BEHAVIOUR DISORDERS IN ADOLESCENCE Vulnerability + Risk factors Symptoms Pronogsis Tretment Clinical diagnosis Therapeutic and Preventive Interventions
GLOBAL AND DEVELOPMENTAL ASSESSMENT OF BEHAVIOUR DISORDERS IN ADOLESCENCE VULNERABILITY + RISK FACTORS SYMPTOMS PROGNOSIS • Genetic factors • Temperament • mediators • Personality traits • Cognitive patterns • Neuropsychology • Neurophysiology • Neurotransmission * Unspecific * Especific: - Sex - Family - School - Social *Developmental symptoms *Clinical symptoms - Diagnostic criteria - Subtypes - Comorbidity * Clinical features * Protective factors * Temperament Mª C. Ballesteros-Alcalde & J.L. Pedreira-Massa (1999)
Comprehensive and Developmental Assessment of Behaviour Disorders in Adolescence/2Vulnerability • Genetic and Temperament factors as mediators • Personality traits: • Aggressiveness • Socialization disorders • Impulsiveness • Hyperactivity • Cognitive patterns: • Hostile attributions • Egocentric • Low and inconsistent problem-solving skills • Inadequate aims
Comprehensive and Developmental Assessment of Behaviour Disorders in Adolescence/3 • Vulnerability: Genetic and Temperament factors as mediators • Neuropsychology: • Low IQ • Language disorders • Attention disorders • Neurophysiology: • Low dermal conductivity • Loe cardiac rating • Neurotransmissions: • Dopamine, noradrenaline • Serotonine
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/3Risk Factors • Parental Factors: • Antisocial and criminal behaviour • Alcoholism • Untoward parent-child interaction: • Harsh punishment • Inconsistent punishment • Poor supervision • Coercitive exchanges (escalted aversive interactions) • Less parental warmth, support and comunication with children
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/4Risk Factors • Family Factors: • Marital discord • Large family size • Birth order • Older siblings with antisocial behaviour • Few family activities
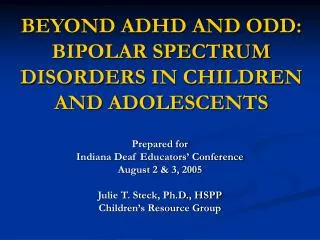
Disruptors of effective parenting Family Demographics Income Parent education Neighborhood Ethnic group Grand parental Traits Antisocial behaviour Poor family management Parental Traits Antisocial behaviour Susceptible to stressors Disrupted family-management practices Child antisocial behaviour Family Stressors Unemployement Marital conflict Divorce B. Lahey & R. Loeber (1994)
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/5Risk Factors • Child Factors: • Child temperament • Neuropsychological deficits (in verbal and executive” functions) • School (academic deficiencies, attendance, peers and teacher relationship) • Signs of antisocial behaviour: Early onset, frequency (number of episodes), diversity (range of different antisocial behaviours), breadth across situations, seriousness
A visual heuristic describing the developmental levels model Mug Truant Cruel Steal Force sex Run away Break, enter Use weapon Lie Bully Vandalize Fight Set fires Hurt animals Temper tantrums Irritable Defiant Spiteful Blame others Annoy others AngryArgumentative Advanced CD Intermediate CD Oppositional B. Lahey & R. Loeber (1994)
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/6Risk Factors • Social Risk Factors: • Poverty • Unemployed • Marginal behaviours or life styles • Migration • Low culture
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/7Symptoms • Diagnostic criteria (symptoms: type, number and frequency) • DSM-IV • ICD-10
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/8Clinical Symptoms • The subtypes of the Disorders • Subtypes based on age at onset • Subtypes based on aggression • Subtypes based on socialization • Subtypes based on comorbid conditions
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/9Clinical Symptoms • Subtypes based on age at onset • Childhood onset vs. Adolescence onset(Longitudinal follow-up study: Farrington, 1979; Dunedin Longitudinal Study; Moffit, 1990 & McGee, 1992)
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/10Clinical Symptoms • Subtypes based on aggression • Overt vs. Covert(1st Bipolar Dimensional Type; Loeber et al, 1985) • Destructive vs. Nondestructive(2nd Bipolar Dimensional Type; Frick et al., 1993) • Proactive vs. Reactive (theoretical model based; dichotomy; Dodge et al., 1991) • Affective vs. Predatory(connection with Autonomous/neurotransmission; Vitello et al., 1990) • Constraint
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/11Clinical Symptoms • Subtypes based on Sociabilization • Socialized vs. undersocialised(Biological functioning is different; Quay et al., 1987)
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/12Clinical Symptoms • Subtypes based on Comorbid Conditions • ADHD • Cognoscitive Disfuctions • Emotional Disorders
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/13Clinical Symptoms • Comorbidity • ADHD • Impulse-control Disorders • Alcohol or Drug abuse • Anxiety, Depression • Sociabilization Disorders
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/14Pronogsis • Clinical Features associated with bad pronogsis: • Age at onset: Childhood • Subtypes of aggression • Destructive • Proactive • Predatory • Sociabilization: Undersocialized • Comorbid conditions: ADHD and/or Cognitive Disfuctions
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/15Pronogsis • Protective Factors: • Higher self-esteemand locus of control • Family support and supervission • Continuity in therapeutic intervention • Early diagnosis and therapeutic intervention • Good accessibility to Child and Adolescent Psychiatric Services • Social support (peer and social context) • School support
Hollistic and Developmental Assessment of Behaviour Disorders in Adolescence/16Pronogsis • Individual Factors: • Temperament • Personality traits • Perception disorder by himself/herself
Assessment of Behaviour Disorders in Adolescence/1 • Diagnostic Assessment: • Obtain patient’s history • Obtain family history • Interview with patient • School information • Physical evaluation AACAP (1997) MªC. Ballesteros; JL Alcázar; JL Pedreira & A de los Santos (1998)
Assessment of Behaviour Disorders in Adolescence/2 • Diagnostic Formulation: • Identify ICD-10/DSM-IV target symptoms • Biopsychosocial stressors, enviromental and developmental factors • Subtype of the Behaviour Disorders • Comorbidity AACAP (1997) MªC. Ballesteros; J.L. Alcázar; J.L. Pedreira & A. De los Santos (1998)
Assessment of Behaviour Disorders in Adolescence/3 • Obtain patient’s history: • Prenatal ahd birth history (substance abuse by mother, maternal infections or medications) • Developmental history (attachment diosrders e.g. Parental depression, substance abuse; temperament, oppositionality, aggression, attention, socialization, impulse control) • Physical/sexual abuse history • History of symptoms development (impact on family and peer relationship, academic problems) • Medical history(CNS pathology, chronic illnesses, somatizations) AACAP (1997); MªC. Ballesteros; J.L. Alcázar; J.L. Pedreira & A. De los Santos (1998)
A developmental progression for antisocial behavior Rejection by normal peers Poor parental discipline and monitoring Commitment to deviant peer group Child conduct problems Deliquency Academic failure Late Childhood and Adolescence Middle Childhood Early Childhood
Multidimensional causal models: Longitudinal model Prior Delinquent Behaviour + Family - Delinquent Behaviour Delinquent Peers + School - Elliot, Huizinga & Ageton (1985) (Condensed & adapted)
Median age Oppositional defiant disorder Conduct disorder 3.0 3.5 4.0 4.5 5.0 5.5 6.0 6.5 7.0 7.5 8.0 8.5 9.0 9.5 10.0 10.5 11.0 11.5 12.0 12.5 13.0 Stubborn Defies adults, temper tantrums. Irritables, argues. Blames others. Annoys others. Spiteful. Angry. Swears. Lies. Fights. Bullies, sets fires. Uses weapon. Vandalizes. Cruel to animals. Physical cruelty. Steals, runs away from home. Truant, mugs. Breaks and enters. Forces sex. Median Age of Onset Reported by Parent of Symptoms of oppositional Defiant Disorder and Conduct Disorder ª ª This combines retrospective and prospective ages of onset over four annual assessment in the Developmental Trends Study. B. Lahey & R. Loeber (1994)
The families of adolescents: The “strop cycle” Harsh criticism from others Identity definition by opposition Precarious self-esteem P. Hill (1992)
Assessment of Behaviour Disorders in Adolescence/4 • Obtain family history: • Family coping style, stressors, resources -socioeconomic status, social support/isolation, problem- solving skills, conflict-resolution skills, parenting skills, limit-setting, abuse/neglect, permissiveness, inconsistency, management child’s aggression, parent’s and patient’s coercitive interaction cycles leading to reiforcement of noncompliance AACAP (1997) MªC. Ballesteros; J.L. Alcázar; J.L. Pedreira & A. De los Santos (1998)
Assessment of Behaviour Disorders in Adolescence/6 • Interview patient (may precede parental interview): • Capacity for attachment, trust and empathy • Tolerance for and discharge of impulses • Capacity for showing restraint, accepting responsability for actions, experiencing guilt,user anger constructively, acknowleding negative emotions • Cognitive functioning AACAP (1997); MªC. Ballesteros; J.L. Alcázar; J.L. Pedreira & A. De los Santos (1998)
Assessment of Behaviour Disorders in Adolescence/7 • Interview patient/2 (may precede parental interview): • Mood, affect, self-esteem, suicide potencial • Peer relationship (loner, popular, drug-, crime-, or gang oriented friends) • Disturbances of ideation (suggestibility, disociation) • History of early, persistent use of tabacco, alcohol or other substances • Psychometric self-report instruments might provide AACAP (1997); MªC. Ballesteros; J.L. Alcázar; J.L. Pedreira & A. De los Santos (1998)
Assessment of Behaviour Disorders in Adolescence/8 • School information: • Functioning (IQ, achievement test data, academic performance and behaviour) • Standard parent and teacher rating scales of the patient’s behaviour • Referral for IQ, speech and language and learning disability and neuropsychiatric testing if available test data are nor sufficient • Data may be obtained inperson, by phone or though written reports from appropiate staff, such as school principal, psychologist, teacher and nurse AACAP (1997); MªC. Ballesteros; J.L. Alcázar; J.L. Pedreira & A. De los Santos (1998)
Cross-Sectional model Parental Monitoring - Deviant Peers - Behaviour problems/ Social Competence + +a Delinquent Behaviour Academic Skills - Patterson & Dishion (1985) (adapted) a: High behaviour problems and low social competence
Assessment of Behaviour Disorders in Adolescence/9 • Physical examination: • Collaboration with family doctor, paediatrician or other health care providers • Vision and hearing screening • Evaluation of medical and neurological conditions (e.g. Head injury, chronic illness) • Urine and blood drugs screening as indicated, especially when clinical evidence suggest substance use AACAP (1997); MªC. Ballesteros; J.L. Alcázar; J.L. Pedreira & A. De los Santos (1998)
Selected Measures of Behaviour Disorders in Adolescents/1 • In order to discriminate clinical and no clinical people: High discriminant reliability • Child Behavior Checklist, Achenbach, 1978 • Revised Behavior Problems Checklist, Quay, 1983 • Eyberg Child Behavior Inventory, Eyberg, 1978 • Conners Rating Scales (Parents and Teachers)
Delinquent behavior Aggressive behaviour Cheats Doesn’t feel guilty Hangs around kids who get in trouble Lies Runs away from home Sets fires Steals at home Steals outside home Swears; uses obscene language Talks or thinks about sex too much Truancy Uses alcohol Uses drugs Vandalizes older kids Argues Brags Bullies; is mean to others Destroys others’ things Demands attention Destroys own things Disobedient at school Jealous Irritable Loud Physically attacks people Screams Shows offor clowns Stars fights Stubborn Sudden mood changes Talks too much Teases other kids Temper tantrums Threatens Achenbach-Connors-Quay Questionnaire (ACQ) delinquent and aggressive behaviour dimensions
Selected Measures of Behaviour Disorders in Adolescents/2 • In order to evaluate the treatment impact: High predictive reliability • Child Behavior Checklist, Achenbach, 1978 • Eyberg Child Behavior Inventory, Eyberg, 1978 • Conners Rating Scales (Parents and Teachers) • In order to require shortness or treatment evaluation or developmental impact: Short Scales • Short’s Conners Rating Scale • Iowa-Conners Teacher Rating Scale • Eyberg Child Behavior Inventory
Selected Measures of Behaviour Disorders in Adolescents/3 • In order to assess behaviour competences or adolescent behaviour profile: • Child Behavior Checklist, Achenbach, 1978 • In order to consider the setting: • Child and Adolescent Psychiatric Services, or comorbidity screening: ABC, CBC, TBP and Conners Scales • Behaviour specific setting: Eyberg Child Behavior Inventory
Family Assessment of Behaviour Disorders in Adolescents/1 • Parenting Profiles: • Parenting Scale (Arnold, 1993) • Parent Practices Scale (Stayhom & Widman, 1998) • Alabama Parenting Questionaire (Frick, 1991) • Parent and Teacher Social Cognitions: • Parenting sense of Competende Scale (Johnston, 1989) • Cleminshaw-Guidubaldi Parent Satisfaction Scale (1985) • Parental Locus of Control Scale (Campis et al., 1986)
Family Assessment of Behaviour Disorders in Adolescents/2 • Parental perceptions of personal and marital adaptation or emotional state: Screening of depressive and mood psychopathology, disocial behaviour and substance or alcohol abuses • Family Stress: • Parenting Daily Hassles (Greener, 1990) • Parenting Stress Index (Abidin, 1995) • Parental functioning in extrafamily context: • Community Interaction Checklist (CIC, Wahler, 1979)
Family Assessment of Behaviour Disorders in Adolescents/3 • Parent conflicts: • O’Leary-Porter Scale (1980) • Conflict Tactics Scale (Partner-Strauss, 1979, 1990) • Parenting Alliance Inventory (Abidin, 1988) • Child Rearing Disagreements (Jouriles et al., 1991) • Parents Problems Checklist (Dadds & Powell, 1991) • Parental satisfaction with treatment procedures: • Parent’s Consumer Satifaction Questionaire (Forehandy & McMahon, 1981; mcMahon, 1984)
Diagnostic Formulation of the Adolescents with Behaviour Disorders/1 • Identify ICD-10/DSM-IV target symptoms • When suggests BD consider the following: • Biopsychosocial stressors (sexual and physical abuse, divorse or death or key attachment figures) • Educational potential, disabilities, achievement • Peer, sibling and family problems and strengths • Enviromental factors (disorganized home, lack of psychiatric illness or drug or alcohol abuse in parents, enviromental neurotoxins e.g. Lead) • Adolescent or Child ego development, especially ability to form and maintain relationships AACAP (1997)
Diagnostic Formulation of the Adolescents with Behaviour Disorders/2 • The subtype of the disorder: • Childhood onset vs. Adolescent onset • Overt vs. Covert versus authority • Under-restrained vs. Over-restrained • Socialized vs. Undersocialized AACAP (1997)
Diagnostic Formulation of the Adolescents with Behaviour Disorders/3 • The syndromes may be confused or cuncurrent with: • ADHD Organic Brain and seizure disorder • ODD Specific developmental disorder • Intermittent explosive disorder Schizophrenia • Substance use disorder Paraphilias • Mood disorder (bipolar and depressive) • PTSD and Disociative disorder Mental retardation • Borderline personality disorder • Somatization disorder Narcisistic personality disorder • Adjustment disorder AACAP (1997)
Dimensional Assessment of Behaviour Disorders in Adolescents/1 • Individual dimensions: • Developmental preocess and moral development • Aggressiveness’ subtypes • Self-esteem and self-likeness • Empathy and impulse control • Comorbility • Poor interpersonal relations • Cognitive and atttributional processes: Deficits and disttorsions in cognitive problem-solving skills, atributions or hostile intant to others, resentment and suspiciousness illustrate • Risk factor and vulnerability • Temperament • Clinical features (specially with sign of antisocial behaviour) AACAP (1997)
Dimensional Assessment of Behaviour Disorders in Adolescents/2 • Family dimensions: • Parenting and attachment styles • Psychopathology (including drug and alcohol abuses) • Untoward parent-child interactions (physical and sexual abuses) • Poor or inconsistent supervision • Marital conflicts • Other family members with antisocial behaviour • Family risk factors • Genetic factors AACAP (1997)
Disruptors of effective parenting Family Demographics Income Parent education Neighborhood Ethnic group Grandparental Traits Antisocial behaviour Poor family management Parental Traits Antisocial behaviour Susceptible to stressors Disrupted family-management practices Child antisocial behaviour Family Stressors Unemployement Marital conflict Divorce B. Lahey & R. Loeber (1994)
Dimensional Assessment of Behaviour Disorders in Adolescents/3 • School dimensions: • Acedemic deficiencies • Neuropsychological deficits (in verbal and “executive” functions) • Behaviour disorder in preschooler’s level • Peer’s relationship and perception of behaviour • Teacher’s supervision and authority AACAP (1997)