Download
1 / 99
990 likes | 1.04k Views
Dive into the world of cortical function through the eyes of neurosurgeon Kathryn Holloway, exploring techniques of cortical mapping, lesional studies, electocorticography, and functional imaging. Discover speech areas, dominance, types of aphasia, and traditional speech regions. Gain insights into left temporal lobe lesions and visual cortex involvement. Explore cases and postoperative outcomes for a comprehensive understanding of cortical function.

E N D
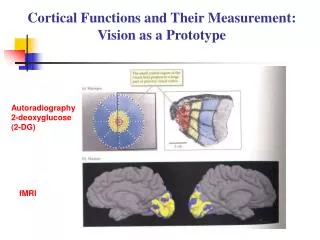
Cortical function as experienced by a neurosurgeon Kathryn Holloway, MD Prof of Neurosurgery
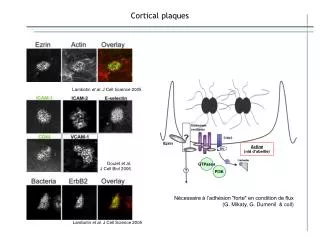
Techniques of Cortical Mapping I Lesional Studies - Correlation of functional deficit with autopsy or Gyral Anatomy on structural imaging studies II Electrocorticography (1) Awake craniotomy (2) Implantation of cortical grid with extraoperative monitoring III Functional Imaging fMRI PET IV MEG magnetic source imaging correlated with MRI
Dominance • In 95% of population the left hemisphere is dominant • Essentially “all” right handed patients with a normal brain are left dominant • A small portion of left handed individuals are right or mixed dominant for speech • Dominance can be assessed by anesthetizing one hemisphere via an intracarotid amytal injection
Types of aphasia • Wernickes • Posterior dominant temporal lobe extending around the angular gyrus into the parietal lobe • Loss of comprehension • Speech tends to be fluid but without content • They are relatively unaware of their deficits • Broca’s • Dominant inferior frontal gyrus • Preserved comprehension • Word generation ability (speech & written ) lost • Patients very aware of deficit and are frustrated
Traditional speech areas Broca‘s Wernickes
Speech • Can, in fact, block naming as well as comprehension in the dominant temporal lobe (Wernicke’s area) • However if there is a comprehension deficit, the lesion is in the dominant temporal lobe • Severe speech production problems without any comprehension problems will be reliably localized to the dominant inferior frontal gyrus
The primary visual cortex is identified on a mid-saggittal cut showing the calcarine fissure
Visual Cortex Visual cortex
G.S. - History 25 year old RH WM working in Poland Onset of right visual field obscurations followed by right homonymous hemianopsia One seizure consisting of a light in the right visual field associated with altered sensation in the right hand
G.S. - Exam No weakness Right homonymous hemianopsia
AVM exposed by retracting brain to see medial surface of hemisphere Area of craniotomy Retracted parietal lobe Falx at midline
AVM exposed by retracting brain to see medial surface of hemisphere Retracted parietal lobe Saggital sinus, falx, midline
Postop angio shows no residual AVM Post-resection angio Pre-resection angio
Damage to secondary association areas give less specific deficits
K.S. - History & Exam 39 year old RH WF Onset of seizures at age 2 Unresponsive to medication Developmentally delayed Normal examination
K.S. - Seizure Types Age 2 - episodes of blindness Age 8 – generalized tonic clonic seizures Teens – sees colors or micropsia or macropsia followed by unresponsiveness with a postictal aphasia Other seizures
The motor/sensory strip can readily be identified on MRI imaging by noting the first vertical gyrus posterior to the horizontal frontal gyri
Distribution of motor/sensory function along central sulcus is well known
F.R. - History 37 year old RH WF Gradual onset of headaches, right sided weakness New onset right sided jerking followed by generalized tonic clonic seizures
F.R. - Exam No aphasia Right sided facial weakness sparing forehead Right arm- spastic paresis Right leg – mild spasticity
Exposure anterior ear Top of head posterior
Resection exposes frontal gyri Motor strip
F.R. - Postoperative Course Resolution of all deficits
In contrast speech and memory function can only be generally localized
Traditional speech areas Broca‘s Wernickes
R.B. - History 14 yo RH WM History of partial complex seizures since the age of 15 months EEG - Left mesial temporal lobe epilepsy with early lateral spread Uncontrolled on Primidone, Tegretol, Dilantin, Valproate, or Tranxene
R.B. - Physical Exam Normal
R. B. – Neuropsychological Evaluation Moderate dominant hemisphere damage
Mesial Sclerosis • Left hippocampus is shrunken and scarred • This is a frequent source of seizures that don’t respond to medication • The dominant temporal lobe is also the area of the brain responsible for verbal memory and speech