Download
1 / 59
640 likes | 866 Views
Treatment of Advanced HER2-Negative Gastroesophageal Carcinomas. David Malka, MD, PhD Head of Gastrointestinal Tumor Group Department of Oncologic Medicine Institut Gustave Roussy Villejuif, France. This program is supported by an educational donation from. About These Slides.

E N D
Treatment of Advanced HER2-NegativeGastroesophageal Carcinomas David Malka, MD, PhDHead of Gastrointestinal Tumor GroupDepartment of Oncologic MedicineInstitut Gustave RoussyVillejuif, France This program is supported by an educational donation from
About These Slides • Our thanks to the presenters who gave permission to include their original data • Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent • These slides may not be published or posted online without permission from Clinical Care Options DisclaimerThe materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials.
Program Faculty Program Director: Manish A. Shah, MDDirector, Gastrointestinal Oncology Weill Cornell Medical College NewYork-Presbyterian Hospital New York, New York Faculty: David Malka, MD, PhDHead of Gastrointestinal Tumor GroupDepartment of Oncologic Medicine Institut Gustave Roussy Villejuif, France
Faculty Disclosures David Malka, MD, PhD, has disclosed that he has received consulting fees from Roche and contracted research support from Amgen, Merck Serono, and Roche. Manish A. Shah, MD, has disclosed that he has received consulting fees and contracted research support from Genentech and sanofi-aventis.
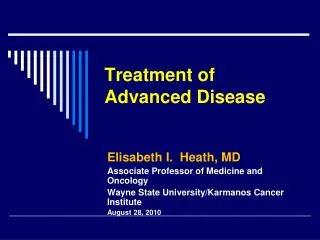
Palliative CT: OS Effective: 11 vs 4.3 mos; P < .00001 Wagner AD, et al. Cochrane Database Syst Rev. 2010;3:CD004064.
Palliative CT « old » « modern » • Taxanes • Oxaliplatin • Oral 5-FU • Irinotecan • 5-FU/antimetabolite • Anthracyclines • Cisplatin + targeted therapies
Palliative CT « old » • FAMTX(5-FU + doxo + HD MTX) • FUP(5-FU + cisplatin) • ECF(epirubicin + cisplatin + 5-FU) • ELF(etoposide + leucovorin + 5-FU) • EAP(etoposide + doxo + cisplatin) • 5-FU/antimetabolite • Anthracyclines • Cisplatin =
Palliative CT « old » • FAMTX(5-FU + doxo + HD MTX) • FUP(5-FU + cisplatin) • ECF(epirubicin + cisplatin + 5-FU) • ELF(etoposide + leucovorin + 5-FU) • EAP(etoposide + doxo + cisplatin) • 5-FU/antimetabolite • Anthracyclines • Cisplatin =
Meta-analysis of Chemotherapy in Advanced Gastric Cancer • PolyCT > single-agent CT • Combination 5-FU/CDDP/anthra > 5-FU/CDDP • Combination 5-FU/CDDP/anthra > 5-FU/anthra Wagner AD, et al. J Clin Oncol. 2006;24:2903-2909. Wagner AD, et al. Cochrane Database Syst Rev. 2010;3:CD004064.
Meta-analysis GASTRIC (Individual Data) Results CT Without vs With Anthracyclines 7 studies = 1195 patients Events/Patients HR & CI CT-anthra CT+anthra CT-anthra CT+ anthra 49 eligible randomized studies (7120 patients) identified A06A13 A15 A17 A20 A24 A26 A29 RothYamamura Cullinan Nio Cullinan Thuss-Pat. Vanhofer Coombes 71/7932/35 60/80 13/27 53/53 44/45 235/251 31/33 30/4137/39176/17616/30103/10340/43115/12530/35 Individual data available for 18 studies (3226 patients): 45% 559/603(92.7%) 553/592(93.4%) 3% ± 6 increase Total Median survival: 8.1 mos 4.0 2.0CT-anthrabetter 1.0 0.5CT+anthra better 0.25 Test for heterogeneityChi-square = 3.73. df = 7; P > .1 HR: 1.03 (95% CI: 0.91-1.17; P = .66) Bouché O, et al. JFHOD 2009. Abstract.
Palliative CT « old » • FAMTX(5-FU + doxo + HD MTX) • FUP(5-FU + cisplatin) • ECF(epirubicin + cisplatin + 5-FU) • ELF(etoposide + leucovorin + 5-FU) • EAP(etoposide + doxo.+ cisplatin) • 5-FU/antimetabolite • Anthracyclines • Cisplatin = Cap-P[1] LV/5-FU2-P[2] 1. Kang Y, et al. ASCO 2006. Abstract LBA4018. 2. Taieb J, et al. Ann Oncol. 2002;13:1192-1196.
PFS (Primary Endpoint) Noninferiority Trial: XP vs FP (ML17032) Medians 5.6 mos (95%CI: 4.9-7.3) 5.0 mos (95% CI: 4.2-6.3) Cisplatin: 80 mg/m² on Day 1 Capecitabine: 2 g/m² on Days 1-14 or 5-FU: 800 mg/m² on Days 1-5 Every 3 wks XP (n = 139) FP (n = 137) 1.0 0.8 0.6 Proportion With PFS 0.4 N = 316 0.2 0 2 4 6 8 10 12 14 16 18 20 22 24 26 0 Mos Kang YK, et al. Ann Oncol. 2009;20:666-673.
Palliative CT Regimens « old » • 5-FU/antimetabolite • Anthracyclines • Cisplatin FUP (XP) ECF (ECX)
Palliative CT « old » « modern » • 5-FU/antimetabolite • Anthracyclines • Cisplatin • Taxanes • Oxaliplatin • Oral 5-FU • Irinotecan FUP (XP) ECF (ECX)
Palliative CT « old » « modern » • 5-FU/antimetabolite • Anthracyclines • Cisplatin • Taxanes • Oxaliplatin • Oral 5-FU • Irinotecan FUP (XP) ECF (ECX)
Tax325 Trial: Phase III Study in First-line Advanced Gastric Cancer Docetaxel75 mg/m2 on Day 1 CDDP 75 mg/m2 on Day 1 5-FU 750 mg/m2 on Days 1-5 q3w R CDDP 100 mg/m2 on Day 1 5-FU 1000 mg/m2 on Days 1-5 q4w N = 457 Primary endpoint: TTP Van Cutsem E, et al. J Clin Oncol. 2006;24:4991-4997.
TAX325: TTP Final Analysis 100 HR: 1.47 (95% CI: 1.19-1.82) Risk reduction: 32% 90 DCF Median: 5.6 mos CFMedian: 3.7 mos Log-rank P ≤ .001 80 70 60 50 Probability (%) 40 30 20 10 0 0 3 6 9 12 15 18 21 Mos Pts at Risk, n DCFCF 148119 7142 4018 1710 105 7 6 Van Cutsem E, et al. J Clin Oncol. 2006;24:4991-4997.
TAX325: Phase III DCF vs CF for Advanced Gastric Cancer Van Cutsem E, et al. J Clin Oncol. 2006;24:4991-4997.
Alternatives to DCF: Less Toxic and as Effective? Some Examples . . . Randomized phase II study (GATE study) of docetaxel plus oxaliplatin with or without fluorouracil or capecitabine in metastatic or locally recurrent gastric cancer. Van Cutsem E, Boni C, Tabernero J, et al. ASCO 2011. Abstract 4018.
Palliative CT Regimens « old » « modern » DCFmDCF • 5-FU/antimetabolite • Anthracyclines • Cisplatin • Taxanes • Oxaliplatin • Oral 5-FU • Irinotecan FUP (XP) ECF (ECX)
Palliative CT Regimens « old » « modern » DCFmDCF • 5-FU/antimetabolite • Anthracyclines • Cisplatin • Taxanes • Oxaliplatin • Oral 5-FU • Irinotecan FUP (XP) ECF (ECX)
E: Epirubicin 50 mg/m2 +C: Cisplatin 60 mg/m2 +F: 5-FUc 200 mg/m2/day REAL2 Trial in Advanced Gastric Cancer ECF EOF O: Oxaliplatin 130 mg/ m2/3 wks Primary endpoint = OS 5-FU vs X Noninferiority ECX EOX X: Capecitabine 1250 mg/m2/day N = 1002 CisplatinvsOxaliplatin Cunningham D, et al. N Engl J Med. 2008;358:36-46.
REAL2: Survival Survival by Regimen (ITT) 100 80 60 ECFEOFECXEOX Probability of Survival (%) 40 20 0 0 1 2 3 Yrs Since Randomization Cunningham D, et al. ASCO 2006. Abstract LBA4017. Cunningham D, et al. N Engl J Med. 2008;358:36-46.
Palliative CT Regimens « old » « modern » DCFmDCF • 5-FU/antimetabolite • Anthracyclines • Cisplatin • Taxanes • Oxaliplatin • Oral 5-FU • Irinotecan FUP (XP) EOX FOLFOX FLO ECF (ECX)
Palliative CT Regimens « old » « modern » DCFmDCF • 5-FU/antimetabolite • Anthracyclines • Cisplatin • Taxanes • Oxaliplatin • Oral 5-FU • Irinotecan FUP (XP) EOX FOLFOX FLO ECF (ECX)
Phase III Strategic Trial: FFCD 03-07 • Primaryendpoint: time to first-line treatmentfailure (TTF1) • Secondaryendpoints • PFS, OS (TTF second line) • Toxicity • ORR, QoL • QLQC30 and STO-22 • Stratified by: • Mesurable or not • WHO PS 0-1 or 2 • Adj (R)CT or not • Linitis or not • Cardial or gastric • Center A: ECX until progression ; FOLFIRI 2d line R B: FOLFIRI until progression ; ECX 2d line ECX : D1 = epirubicin 50 mg/m² (15 min), cisplatin 60 mg/m² (1 hr); D2-15 : capecitabine 1 g/m² x 2/day; D1 = D21Cumulated dose of epirubicin < 900 mg/m² (max 18 cures)FOLFIRI: D1 = irinotecan 180 mg/m² (90 min) + LV 400 mg/m² (2 hrs), 5-FU b 400 mg/m², 5-FU ci 2400 mg/m² (46 hr). D1 = D14 Time fromrandomization to: 1/progression or 2/treatment interruption or 3/death Guimbaud R, et al. ESMO 2010. Abstract 8010.
FFCD 03-07: TTF1 ECX first line: 4.24 mos (95% CI: 3.48-4.65) FOLFIRI first line : 5.09 mos (95% CI: 4.53-5.68) 1.0 0.8 Less toxicity with FOLFIRI Log-rank P = .008 HR (ECX vs FOLFIRI): 0.77 (95% CI: 0.63-0.94) 0.6 TTF OS: ECX first line: 9.49 mos FOLFIRI first line: 9.72 mos 0.4 0.2 0 = 32 0 4 8 12 16 20 24 28 Mos ECX 209 108 33 8 4 2 1 1 1 FOLFIRI 207 123 50 19 6 3 2 1 0 Guimbaud R, et al. ESMO 2010. Abstract 8010.
Palliative CT Regimens « old » « modern » DCFmDCF • 5-FU/antimetabolite • Anthracyclines • Cisplatin • Taxanes • Oxaliplatin • Oral 5-FU • Irinotecan FUP (XP) EOX FOLFOX FLO ECF (ECX) IF FOLFIRI
Targeted Agents for First-line Treatment of Advanced Disease
Targeting VEGF in Gastric Cancer • VEGF is a key mediator of angiogenesis[1] • VEGF expression is associated with more aggressive disease and poor prognosis in gastric Ca[2,3] • Bevacizumab: • Antibody against VEGF 1. Neufeld G, et al. FASEB J. 1999;13:9-22. 2. Kim SE, et al. Gut Liver. 2009;3:88-94. 3. Lieto E, et al. Ann Surg Oncol. 2008;15:69-79.
AVAGAST International, phase III, advanced gastric ADK, first line (n = 774) CDDP (x6)–capecitabine (or FU) + bevacizumab or placebo • Subgroup analyses (planned): Americas > Europe > Asia • No unexpectedtoxicity • Benefit • PFS (6.7 vs 5.3 mos; HR: 0.80; 95% CI: 0.68-0.93; P = .004) • ORR (46.0% vs 37.4%; P = .03) Bevacizumab: active, but variable according to region – cancer biology? biomarker? 1.0 Fluoropyrimidine/cisplatin + placeboFluoropyrimidine/cisplatin + bevacizumab 0.9 0.8 0.7 HR: 0.87(95% CI: 0.73-1.03;P = .100) 0.6 12.1 Survival (probability) 0.5 0.4 10.1 0.3 0.2 0.1 0 0 3 6 9 12 15 18 21 24 Mos Since Start of Study Patients at Risk, nFluoropyrimidine/cisplatin + placeboFluoropyrimidine/cisplatin + bevacizumab 387387 343355 271291 204232 146178 98104 5450 1519 00 Ohtsu A, et al. J Clin Oncol. 2011;30:3968-3976.
AVAGAST Nonasiatic patients, diffuse or distal gastric adenocarcinoma OS (%) 1.0 Placebo + chemotherapy 0.9 Bevacizumab + chemotherapy 0.8 0.7 0.6 0.5 0.4 0.3 0.2 HR: 0.67(95% CI: 0.52-0.88) 0.1 0 0 3 6 9 12 15 18 21 24 Mos Patients at Risk, nPlacebo + chemotherapyBevacizumab + chemotherapy 163159 134144 94119 6394 4363 2528 910 13 00 Shah MA, et al. ASCO GI 2012. Abstract 5.
AVAGAST: Potential Predictive Markers for Efficacy of Bevacizumab in Gastric Cancer • High baseline plasma VEGF-A and low baseline neuropilin-1 expression each associated with trend toward improved OS with bevacizumab • Significant benefit observed in pts from non-Asian geographic regions *High indicates > median value; low indicates l≤ median.†PFS during first-line therapy.‡For bevacizumab + chemotherapy vs placebo + chemotherapy.§Interaction of treatment effect using likelihood ratio test. Van Cutsem E, et al. J Clin Oncol. 2012;[Epub ahead of print].
Targeting EGFR in Gastric Cancer EGFR Overexpression: > 50% KRAS/BRAF mutations: rare
Anti-EGFR • 30% to 90% of gastric cancers: EGFR overexpression 1. Lordick F, et al. Br J Cancer. 2010;102:500-505. 2. Moehler M, et al. Ann Oncol. 2011;22:1358-1366. 3. Pinto C, et al. Br J Cancer. 2009;101:1261-1268. 4. Pinto C, et al. Ann Oncol. 2007;18:510-517. 5. Kim C, et al. Invest New Drugs. 2011;29:366-373. 6. Han SW, et al. Br J Cancer. 2009;100:298-304. 7. Richards DA, et al. ASCO 2011. Abstract 4015. 8. Woell E, et al. ASCO 2009. Abstract 4538. 9. Chan JA, et al. Ann Oncol. 2011;22:1367-1373. 10. Li J, et al. ASCO 2010. Abstract 4107.
Targeting EGFR in Gastric Cancer EGFR • Cetuximab: EXPAND[1] • XP vs XP + cetuximab • Completed, n = 870 (endpoint: PFS) • Panitumumab: REAL3[2] • EOX vs EOX + panitumumab 1. ClinicalTrials.gov. NCT00678535. 2. Waddell TS, et al. ASCO 2012. Abstract LBA4000.
REAL3: Trial Design EOCE 50 mg/m2, O 130 mg/m2+ C 1250 mg/m2/day (n = 275) Untreated advanced adenocarcinoma or undifferentiated carcinoma of the esophagus, OGJ, or stomach (N = 553) mEOC+ PE 50 mg/m2, O 100 mg/m2+ C 1000 mg/m2/day + P 9 mg/kg (n = 278) 1:1 R Waddell TS, et al. ASCO 2012. Abstract LBA4000.
REAL3: Outcomes • In the mEOC arm, grade 1-3 rash was associated with: • Improvement in median OS 10.2 vs 4.3 mos (P < .001) • Similar significant improvements seen in RR and PFS • Multivariate analysis for OS in the first 200 patients has not revealed other predictive markers associated with panitumumab • Multivariate analysis for OS showed a negatively prognostic role for KRAS mutation (P = .025) and PI3KCA mutation (P = .048) Waddell TS, et al. ASCO 2012. Abstract LBA4000.
Targeting HGF/c-Met Pathway • HGF/c-Met pathway: mediates mitogenesis, morphogenesis, and motogenesis[1] • Over or aberrant expression of HGF or c-Met reported in various human cancers, including gastric[2] • Rilotumumab[3] • Human IgG2 monoclonal antibody directed against human HGF • Blocks HGF binding to its receptor c-Met • Inhibits cell activities mediated via HGF/c-Met path (cell proliferation, survival, migration, and invasion) 1. Birchmeier C, et al. Nat Rev Mol Cell Biol. 2003;4:915-925. 2. Peruzzi B, et al. Clin Cancer Res. 2006;12:3657-3660. 3. Giordano S. Curr Opin Mol Ther. 2009;11:448-455.
First-line CT: Rilotumumab ECX +Rilotumumab 15 mg/kg/3 wks (n = 40) Phase II LA/M+ Gastric/GEJ PS 0-1 (N = 121) ECX + Rilotumumab 7.5 mg/kg/3 wks (n = 42) R ECX + Placebo (n = 39) • primary endpoint: PFS • secondary endpoints: ORR, OS, toxicity, biomarkers Iveson T, et al. ESMO 2011. Abstract 6504.
First-line CT: Rilotumumab Iveson T, et al. ESMO 2011. Abstract 6504.
First-line CT: Rilotumumab Biomarker population (n = 90) • In ECX + placebo arm, high c-Met associated with shorter OS vs low c-Met • HR: 3.22 (95% CI: 1.08-9.63) Oliner KS, et al. ASCO 2012. Abstract 4005.
First-line CT: Rilotumumab Iveson T, et al. ESMO 2011. Abstract 6504.
MEGA: Ongoing Trial PRODIGE 17 ACCORD 20/0904 MEGAFrench, multicenter, open-label, randomized phase II trialEudract N°: 2009-012797-12 Endpoints • Primary: 4-mo PFS rate (RECIST 1.1) • Secondary: toxicity (NCI CTC AE V4), objective response rate, disease control rate, TTP, PFS, OS • Exploratory • Pharmacogenetic analyses • EGFR/RAS/RAF and HGF/c-Met pathway analyses • Circulating tumor/immune cell levels • AGEC (n = 165)First linePS 0-1Stratified by: • Stage (LA vs M+) • Type (signet-ring cell/diffuse vs intestinal/mixed) • Center (n ~ 30) mFOLFOLX6*(n = 55) Until disease progression or limiting toxicity mFOLFOLX6* + Panitumumab†(n = 55) R mFOLFOLX6*+ Rilotumumab‡(n = 55) *Oxaliplatin 85 mg/m2 in 2 hrs, folinic acid 400 mg/m2 in 2 hrs, fluorouracil 400 mg/m2 bolus then 2400 mg/m2 in 46 hrs, every 2 wks. †6 mg/kg IV in 1 hr, every 2 wks.‡10 mg/kg IV in 1 hr, every 2 wks. Malka D, et al. ASCO 2011. Abstract TPS178.
Second-line CT: First Phase III Trial BSC (n = 69) Phase III 1 or 2 CT lines (5-FU/platinum) PS 0-1 (N = 202) R 2:1 Docetaxel 60 mg/m2/3 wks Or Irinotecan 150 mg/m2/2 wks CT + BSC (n = 133) • Primary endpoint: OS Kang JH, et al. J Clin Oncol. 2012;30:1513-1518.
Second-line CT: First Phase III Trial • Medianage: 56 yrs • 1 line: 73%; 2 lines: 27% • PS 0: 54% • > 1 M+ site: 65% • < 3-mo treatment-free interval: 74% • Further CT, ≥ 3rd line: 40% vs 22%;P = .011 • No QoL data Kang JH, et al. J Clin Oncol. 2012;30:1513-1518.
Second-line CT: First Phase III Trial 1.0 CT + BSCBSC 0.8 0.6 Survival Probability 0.4 0.2 0 0 3 6 9 12 15 18 21 Mos Pts at Risk, n CT + BSCBSC 13369 10145 6415 3611 267 185 Kang JH, et al. J Clin Oncol. 2012;30:1513-1518.
Palliative CT Regimens « old » « modern » DCFmDCF • 5-FU/antimetabolite • Anthracyclines • Cisplatin • Taxanes • Oxaliplatin • Oral 5-FU • Irinotecan FUP (XP) EOX FOLFOX FLO ECF (ECX) IF FOLFIRI Targeted therapies
Targeted Agents for Second/Third-line Treatment of Advanced Disease
Targeting PI3K/mTOR Pathway in Gastric Cancer • PI3K/mTOR pathway: important regulator of cell growth, survival, proliferation, angiogenesis, and metabolism • 50% to 60% of gastric cancers demonstrate dysregulation of the pathway[1-3] • mTOR inhibitors demonstrated preclinical and early clinical efficacy in gastric cancer[1,4-7] 1. Xu DZ, et al. BMC Cancer. 2010;10:536. 2. Lang SA, et al. Cancer. 2007;120:1803-1810. 3. Yu G, et al. Clin Cancer Res. 2009;15:1821-1829. 4. Taguchi F, et al. Invest New Drugs. 2011;29:1198-1205. 5. Cejka D, et al. Anticancer Res. 2008;28:3901-3908. 6. Jaeger-Lansky A, et al. Cancer Biol Ther. 2010;9:919-927. 7. Doi T, et al. J Clin Oncol. 2010;28:1904-1910.