Download
1 / 40
400 likes | 410 Views
The Promise of Epigenetic Therapy in Solid Tumors: DNA Methylation Inhibitors in Testicular Cancer. Michael J. Spinella University of Illinois September 27, 2017. Outline Background on TGCTs In vitro findings with decitabine in TGCTs Pre-clinical and translational studies Clinical trial.

E N D
The Promise of Epigenetic Therapy in Solid Tumors: DNA Methylation Inhibitors in Testicular Cancer Michael J. Spinella University of Illinois September 27, 2017
Outline • Background on TGCTs • In vitro findings with decitabine in TGCTs • Pre-clinical and translational studies • Clinical trial
Testicular Germ Cell Tumors (TGCTs) • Seminoma, nonseminoma (embryonal carcinoma, yolk sac carcinoma, choriocarcinoma, teratoma) • Most common carcinoma of males 15-35 yrs of age • Molecular basis is poorly understood. No tumor suppressor genes consistently mutated, no oncogenes consistently amplified. • Thought to arise from malignant conversion of PGCs • TGCT are highly aggressive solid tumors, but curative with cisplatin-based therapy, (up to 80% cure rate)
Clinical Relevance • Cures come with acute and long-term toxicities including increased risk of secondary malignancies • In addition, patients refractory to cisplatin-based chemotherapy continue to have a very poor prognosis, as do patients who undergo late relapse. Cancer Specific Survival of Late Relapse According to Previous Chemotherapy O’Shaghnessy et al Urol Clin N Am 2015
EC is the stem cell of TGCTs Testicular EC and ES share lots of similarities Embryonal Carcinoma: a pluripotent cancer stem cell Masters and Köberle, 2003
Pathogenesis of testicular germ cell tumors in relation to germ cell origin and age Rajpert-De Meyts et al Lancet 2016
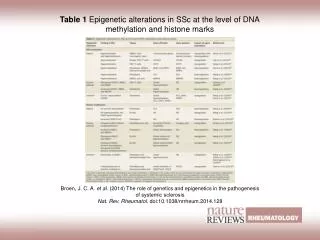
Reprogramming of DNA methylation during the male germ cell cycle TGCT Origin Evidence for distinct patterns of DNA methylation in TGCT compared to cancers of somatic tissue origin
DNA Methylation DNMT1 = maintenance methyltransferase DNMT3A, DNMT3B = de novo methyltransferase
TGCT cells express much higher levels of DNMT3B protein than somatic tumor cells Beyrouthy et al Cancer Res 2009
Effect of 5-aza-CdR on TGCTs and somatic cells 120 Cell number (%) 100 80 * * 60 * * 40 * * * * * * 20 0 10 1000 0 100 Guadecitabine (nM) Biswall et al Plos One 2013
DNMT3B knockdown (shRNA) results in resistance to 5-aza Cell number (%) 120 NT2/D1 100 * 80 DNMT3B expression * * 60 * * 40 * * * * 20 * * 0 10 50 0 2.0 5.0 100 Drug (nM) Biswall et al Plos One 2013
Pretreatment with low-dose 5-aza-CdR restored cisplatin sensitivity to cisplatin-resistant EC cells. Beyrouthy et al Cancer Res 2009
Low 5-aza-CdR activates ATM pathway and expression of methylated genes Beyrouthy et al Cancer Res 2009
Low dose 5-aza induces an early, robust and unique reprogramming of gene expression and DNA demethylation in EC cells 1) Induction of p53 target genes, 2) Induction of genes known to be repressed by methylation 3) repression of pluripotency genes Biswall et al Plos One 2013
Confirmation of promoter demethylation with low dose 5-aza in EC cells 1) Induction of p53 target genes, 2) Induction of genes known to be repressed by methylation 3) repression of pluripotency genes Biswall et al Plos One 2013
Translational Studies -TGCT are highly curable with cisplatin-based therapy but resistance does occur at 10-20% of patients die of disease. No effective therapies for these patients. No prognostic markers to predict non-responders. -Dr. Costa Albany from Indiana contacted us to propose a collaboration to conduct a clinical trial. -Hypothesis = TGCTs are curable because of hypomethylation. Cisplatin resistance may be due to increased methylation that is reversible with DNA methylation inhibitors.
SGI-110 (Astex pharmaceuticals) (guadecitabine) Resistant to cytidine deaminase
Low dose SGI-110 dramatically inhibits cisplatin resistant EC growth in vivo SGI110 start SGI110 end Albany et al Oncotarget 2017
Low dose SGI-110 dramatically inhibits cisplatin resistant EC growth in vivo Albany et al Oncotarget 2017
Low dose SGI-110 resensitizes cisplatin resistant EC in vivo Drug Start Drug End Tumor Volume (mm2) Time (days) Albany et al Oncotarget 2017
SGI-110 induced p53 and immune pathway gene expression signatures in EC tumors Albany et al Oncotarget 2017 Hallmark p53 Pathway Hallmark_Allograft_Rejection Hallmark_TNFASignaling_Via_NFKB NES = 2.35 NES = 1.85 NES = 2.64 SGI-110 Control Control SGI-110 Control SGI-110
Phase 1b single arm safety and dose finding trial for refractory testicular germ cell tumor patients (NCT02429466) Endpoints: Global tumor DNA methylation, global tumor gene expression, DNMT3B expression, pyrosequencing -Dr. Costa Albany Indiana University School of Medicine
Two complete responders (NCT02429466) Metastatic TGCT 1st line BEPx4 2nd line HDCT TI-CEx3 3rd line Brain Radiation 4th line SGI-110 + cisplatin Metastatic PMNSGCT 1st line VIPx4 2nd line HDCT x2 3rd line GemOX x 2 4th line SGI-110 + cisplatin Before Before After After HCG AFP Of first 7 patients entered, two had a complete response, two had a partial responses and one is still on therapy.
Clinical Impact Potential salvage therapy for cisplatin-resistant TGCTs Potential to be a shared feature with solid tumor cancer stem cells? Hypothesis on Curability of TGCTs Pluripotent “open” chromatin (potentially via hypomethylation) renders TGCTs uniquely sensitive to DNA damaging agent-induced transcription programs (like via p53) Increased DNA methylation may be a mechanism of cisplatin resistance in TGCTs Demethylating agents like 5-aza may resensitize these patients to cisplatin Understanding these mechanism will inform epigenetic-based therapies for refractory testicular cancer and other solid tumors
Future Directions-Mechanisms of 5-aza hypersensitivity • Induce expression of endogenous retroviruses and innate immune response • TGCT specific non CpG methylation in gene bodies mediated by DNMT3B • Promoter demethylation and tumor suppressor gene expression • DNA adducts and DNA damage response
Future Directions-Clinical • Phase I trial is continuing. We are obtaining pre- and post SGI-110 treaded biopsies for molecular analysis 2. Planed cooperative-based, randomized phase II efficacy trial comparing SGI 110 + cisplatin vs cisplatin alone in relapse/refractory patients 3. Conducting a retrospective methylation study in sensitive and relapsed TGCT patients. 4. Dr. Robert Pili from Indiana University is making PDX models from the phase I patient samples 5. Plans to conduct Immune checkpoint inhibitor + SGI-110 in TGCT patients
Acknowledgements Lab (current) - Emmanuel Bikorimana • Ema Khan • Jennifer Rodriquez • Andrea Corbet • Nichole Sidebotham Lab (former) • Maroun Beyrouthy • Bijesh Biswal • Mary Hever • Pingping Mao • Christina Yim UIUC -Sarah Freemantle -Alyssa Steege -Katrina Gerhard Dartmouth - Brock Christensen Indiana University -Costantine Albany -Lawrence Einhorn -George Sandusky Supported by NIH, ACS, Lance Armstrong Foundation, DOD, Alex Lemonade Stand
Retrospective Study Brock Christensen Kevin Johnson Unsupervised clustering of CpG DNA methylation of 23 archival FFPE TGCTs. Top 10,000 most variable CpG sites were used to cluster the 23 samples. Yellow is hypomethylation, blue is hypermethylation. Green bar denotes cases with curative response to cisplatin, Red are cases resistant to cisplatin therapy. Histology code is EC, embryonal carcinoma; Sem, seminoma; Ter, teratoma; YS, yolk sac tumor; Mixed, mixed nonsemioma and seminoma.
Retrospective study and phase I Trial Goal: Provide rationale for a cooperative-based, randomized phase II efficacy trial comparing SGI-110 + cisplatin vs cisplatin alone in relapse/refractory patients Future Directions for Individualized Treatments for GCT • Predict tumor behavior by molecular methylome signatures • Patient prognosis • Stratify patients into risk categories by clinical/molecular parameters • Predict disease recurrence and cancer-related death • Select treatment approach and predict response • Based on the target expression • Minimize unnecessary exposure to treatment toxicity
Retrospective Study 1. To determine whether tumor hypermethylated is associated with cisplatin resistance 2. To determine whether poor risk TGCTs are hypermethylated compared to good risk TGCTs Endpoints: 450K DNA methylation array 30 gene nanostring panel (DNMTs, Biomarkers) DNMT3B IHC Pyrosequencing, LINE candidate biomarkers from array.
SGI-110 activity in EC cells depends on p53 Cell number (%) * 120 * 100 p53 expression * 80 60 40 * 20 0 0 10 20 50 0.5 5.0 2.0 Guadecitabine (nM)
Low dose 5-aza induces active ATM and H2AX even in DNMT3B KD cells
Plasma Decitabine compared with SGI-110 Decitabine exposure window after SQ injection of SGI-110 is prolonged compared to previously published data of decitabine IV infusion
SGI-110 induces immune pathway gene expression signatures in EC tumors HLA-A HLA-F HLA-CG4 HLA-G HLA-CP5 Expression Expression Expression Expression Expression SGI-110 Cont Cont SGI-110 Cont Cont SGI-110 SGI-110 Cont SGI-110 NKRF NFKBIA TNFSF9 NFKBIZ NKFB2 Expression Expression Expression Expression Expression Cont SGI-110 Cont Cont SGI-110 Cont SGI-110 SGI-110 SGI-110 Cont Relative gene expression * * *
SGI-110 treated Vehicle treated
Proposed distinctive patterns of DNA methylation among TGCT, normal cells and cancers of somatic tissue origin
Brief Summary -Testicular germ cell tumor (TGCT) cells are highly sensitive to very low (10 nM) decitabine (1,2). -The hypersensitivity is correlated with and depends on very high levels of DNMT3B. -Mechanism is associated with global DNA-damage associated p53 activation, anti-pluripotency and demethylation and re-expression of tumor suppressor genes. -Cisplatin resistant TGCT cells are were equally sensitive to decitabine and decitabine could restore their sensitivity to cisplatin. -Recent studies confirm our major findings (3,4).