Download
1 / 15
170 likes | 917 Views
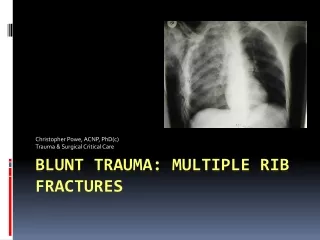
Multiple Trauma. Cindy Fehr Fall 2005. Trauma. Blunt or penetrating external force exerted on the body resulting in injury leading cause of death within first 45 years of life in Canada If not death, major cause for permanent disability

E N D
Multiple Trauma Cindy Fehr Fall 2005
Trauma • Blunt or penetrating external force exerted on the body resulting in injury • leading cause of death within first 45 years of life in Canada • If not death, major cause for permanent disability • Costs society in terms of lost productivity, hospital days and life-long health care costs (11% total cost of health care) • Largely preventable
Background • Trauma not new concept – as long as there has been conflict, there has been trauma, injury & death as a result • Trauma care more focus since Vietnam war – focus on immediate management for better patient outcomes • Continual research re value in lessening emergency response time and minimizing death & disability rates as a result of health care interventions • Trauma is complex and requires timely, coordinated treatment
Epidemiology • Blunt trauma • associated with acceleration, deceleration, shearing, compression forces • Traffic accidents, falls, sports injuries, explosions • Most common cause of traumatic injury • Penetrating trauma • Due to object injuring skin, tissue, underlying organs, viscera, bone • Any sharp object - knife, bullet, broken glass, impalement
Traumatic Deaths • Occur in three ‘peak’ times • Trauma care focused on preventing deaths and minimizing disability during these peaks • Involves early recognition of life-threatening injuries, prompt treatment by appropriately trained health professionals
First Peak • Within seconds/minutes of injury • Due to overwhelming & unsalvageable injuries • Major vessel, brain or very high spinal cord injury Prevention – avoid injury from occurring altogether (seat belts, air bags, helmets, education re safety initiatives)
Second Peak • Minutes to hours after injury • Due to hypoxia (and resulting acidosis), blood loss, hypovolemia, clotting disorders, severe head injuries Prevention – rapid emergency response; quick assessing, resuscitating & getting to OR
Third Peak • Hours, days or weeks after injury • Due to complications from hypothermia, clotting disorders, sepsis, organ failure Prevention – identify & treat potential problems & prevent secondary injury
Primary Survey • Initial assessment & resuscitation • Identify and quickly correct any life-threatening or limb-threatening injuries • Completed in organized and sequential method (vertical organization) • Each member of the trauma team has specific roles and responsibilities (horizontal organization) • X-rays, lavages, CT scans
ABCDE & AMPLE A – airway with spinal precautions B – breathing and ventilation C – circulation and control of deadly bleeding D – disability and dysfunction E – exposure & environmental control A – allergies M – medications P – pertinent past medical history L – last food/drink E – events leading to injury
Secondary Survey • Once hemodynamically stable – sometimes only after OR & in ICU • To look for other less threatening injuries • Includes CWMS of extremities • Less obvious & life-threatening musculoskeletal system injuries identified (deformities, hematomas, open wounds, ecchymosis, painful areas)
Other Considerations • Once neurological injury ruled out, can more easily medicate for pain can impact oxygenation, stabilization of injuries, can signal complication, recover quicker with adequate control • Keep family/significant contact informed • Document, document, document
Potential Complications • Hypovolemia • Hypothermia • Acidosis • DIC (consumptive coagulopathy) • Sepsis • DVT & PE • Compartment Syndrome • Fat Embolism • Rhabdomyolysis (discussed in later wks)