Download
1 / 33
330 likes | 402 Views
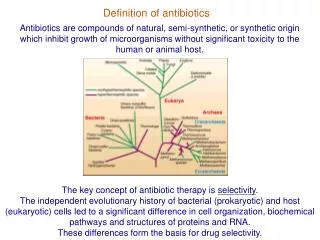
Definition of obesity. Obesity is a chronic disease without tendency towards spontaneous recovery in which a clinical syndrome is produced by the following factors: extrinsic:

E N D
Definition of obesity Obesity is a chronic disease without tendency towards spontaneous recovery in which a clinical syndrome is produced by the following factors: • extrinsic: • abnormal eating pattern, overproduction of food, low level of physical exercise (urbanization, car transportation), stress, emotional disorders • intrinsic: • genetic, metabolic, regulatory, degenerative WHO. Obesity: Preventing and Managing the Global Epidemic. WHO/NUT/NCD/98.1Report of a WHO consultation on Obesity, Geneva, 1998
Prevalence od obesity in Europe (WHO MONICA study), USA and Australia USA** Europa* Australia* 50 45 Men 40 Women 35 30 25 20 15 10 5 0 UK Italy Spain Russia Whites Whites France Finland Poland Sweden Belgium Hungary Maorees Denmark Lithuania Germany Afro-Amer Switzerland Czech Republic *BMI >30 kg/m2; **BMI >27.3 kg/m2 (women), >27.8 kg/m2 (men)
Predicted prevalence of obesity and overweight in the year 2010 Overweight BMI 25 - 29.9 Obesity BMI 30 -39.9 Obesity BMI > 40 100 80 60 40 20 0 Italy UK France Spain USA Germany
ENERGY BALANCE Energy expenditure Food intake Controlling factors Everyday activity Basic metabolic rate Food induced thermogenesis Genetic Diet components Psychologic Social, cultural
Obesity-related diseases Stroke Hypertension Heart failure Respiratory diseases (SAS) Breast cancer CHD, arrhythmia Diabetes Gall bladder diasease Osteoarhrosis Hormonal disturbances Cancer of the colon, endometrium, ovary, prostate Venous insufficiency Gout
Weight (kg) Height (m2) BMI = Classification BMI (kg/m2) Health hazard Normal range 18.524.9 Avarage Overweight (Class I obesity) 25.029.9 Moderate Class II obesity 30.039.9 Serious Class III obesity (morbid) 40.0 Extremely serious World Health Organization, 1998 Obesity is diagnosed using body mass index (BMI)
When BMI is not used in diagnosing obesity? • In children • In sportmen, athletes • In pregnant and breast-feeding women • In the elderly
First of all, obesity is ... • Excessive accumulation of fat tissue • > 10-15% of body weight in men > 20-25% of body weight in women • Different distribution abdominal obesity femoro-gluteal obesity
How to assess body fat distribution? • Waist circumference measurement (half the distance between lower costal margin and upper margin of iliac crest) • Hip circumference measurement (at the level of trochanter major of the femur) • Waist to hip ratio determination (WHR) WOMEN: WHR > 0.8 - abdominal (visceral) obesity MEN: WHR > 1.0
cm Waist circumference is a good indicator of visceral fat and the risk of obesity-related complications ... Women Men 80 cm = increased risk1 >88 cm = health problems 94 cm = increased risk1 >102 cm = health problems 1Lean MEJ, et al. Lancet;1998:351:853–6
History taking • body weight from childhood, through puberty to adult life (studies, marriage, pregnancy, menopause); the pattern of body weight increase, circumstances of weight increase • obesity in family members (genetic factors) • eating habits and behaviour in the family : - response to stress, positive and negative emotions, - binge episodes - physical activity (enviromental factors) - alcohol, cigarettes • previous attempts to reduce body weight (success, failure, relapse)
DRUG-INDUCED glucocorticoids phenotiazines sedativa estrogens progesterone insulin sulphonylureas ENDOCRINOPATHIES Cushing’s sydrome hypothyroidism PCO-S pseudohypoparathyroidism primary hyperinsulinism hypopituitarism CNS DEMAGE trauma, surgery tumours, inflammation, postpartum Turner`s sy Down`s sy GENETIC Prader-Willi sy (15q11) Laurence-Moon-Biedel sy (16q21) Differential diagnosis – secondary obesity
WHO IS AT RISK? All overweight and obese patients including children and adults up to 65 years of age • HOW TO ASSESS THE RISKS? • BMI • waist circumference • (visceral body fat =independent factor of increased mortality) • genetic risk factors • enviromental risk factors • concomittant diseases • general health status
Physical examination - hints • Symptoms and conditions associated with obesity - quality of life - arterial hypertension; exercise tolerance - other cardiovascular disease - diabetes - dyspnoea, snoring, morning somnolence, headache - menstrual disturbances, uterine bleeding, infertility, impotence - back pain, leg pain, pitting oedema - gall stones, pyrosis - constipation
Physical examination - hints - RR, heart rate - dyspnoea (resting, on exertion); cyanosis; anasarca - skin (dry, striae, acantosis nigricans, candidiasis) - body hair distribution; breast examination - thyroid gland - lower lung borders - cardiac sillhouette - liver - joints - lower limbs: varicose veins
Laboratory and imaging studies - ECG, exercise ECG - fasting and postpradial (2 h) glucose - triglicerides - blood gases analysis * - breast X-ray and US - transvaginal US (endometrium, ovaries) - gynaecological examination - abdominal US, rectosigmoidoscopy *
The role of a physician in the long-term obesity management • Evaluation of indications for treatment • Setting realistic goals according to: - previous attempts of dieting and physical exercise -physical capacity assessment - social and enviromental status assessment - initial assessment of patient’s personality • Evaluation of indications and contraindications for drug and surgical treatment • Professional supervision of „patients` support groups”
The aim ofobesity management • Prevention of further weight gain • Risk factors reduction • Maintenance of weight reduction at least by 5 - 10%
The benefits of modest weight reduction (-10kg) • Fasting glucose 50% • Total cholesterol 10% • LDL-cholesterol 15% • Triglicerides 30% • Platelet aggregation • Fibrinolysis • Menstrual disturbances 30% • Overall mortality 20% • Deaths related to diabetes 30% • Deaths related to hypertension 40%
Whom to treat? • Patients with BMI > 30 kg/m2 • who agreed to be treated • with metabolic and genetic risk factors • with obesity-related conditions • with obesity-related social and psychological problems
What should be remembered? • Physiological ageing process favours fat accumulation • In patients aged > 65 years no significant relationship between obesity and increased mortality was shown • Gynoid obesity is not associated with serious metabolic consequences • Excessive calorie intake may be a way of „coping with life”
Contraindications for obesity treatment • Absolute : - terminal diseases • Temporary: - pregnancy, breast-feeding - unstable clinical status - psychiatric disorders • Relative: - age > 65 years, - gall stones
Obesity management current concepts • Diet • Physical activity • Behavioural modification (lifestyle, eating pattern) • Social and psychological support • Drugs • Surgery
Daily calorie requirement and actual calorie intake 24-h energy expenditure ~ 25 kcal/kg b.w. Energy requirement = body weight x 25 kcal/24 h What is an average calorie intake during last 7 days?
How to calculate daily calorie intake to reduce body weight by 0.5 - 1.0 kg/week ... METHOD EXAMPLE 1 EXAMPLE 2 Weight, sex, age 100 kg, 45 yrs., M 80 kg, 45 yrs., F Daily energy requirement 2500 kcal 2000 kcal Deduct 600 kcal or 30% 1900 kcal 1625 kcal 1400 kcal 1400 kcal
Even little physical activity is better than no physical activity ... • causes additional energy expenditure • increases exercise capacity • prevents FFM during dieting • increases postprandial thermogenesis • increases sympathetic activity • prevents BMR reduction after weight loss • prevents „rebound phenomenon” • improves mood, fights stress
What should be remembered ? • Physical activity leads to weight reduction but it is a slow process! • The obese are not capable of intensive exercise due to diminished physical capacity. • Lack of time and lack of approval for intensive exercise prevent the increase in physical activity. • Typical recommendation (NHLB Institute, Betehesda): 45 min briskly walking daily for 6 days a week.
Diet and behavioural modification may not be sufficient! • Diet alone • 75% of patients – weight regain after 1 year • Diet and behavioural modification • 71% of patients – weight regain after 2 years • Dieta and behavioural modiication + increased physical activity • 58% of patients – weight regain after po 2 years Safer DJ. South Med J. 1991;84:1470–1474.
Indications for drug treatment • failure of diet modification and increased physical activity • BMI > 30 kg/m2 • BMI < 30 kg/m2 + 1 complication of obesity
Currently approved obesity drugs • sibutramine (Meridia - Abbott): centrally-acting drug; inhibitor of synaptic serotonin and norepinephrine re-uptake • orlistat (Xenical - Roche): pancreatic lipase inhibitor; reduces fat absorption by 30%
START 3 months No reduction by 10% Pharmacology NO SUCCESS Diet Behavioural modification Physical activity SUCCESS Check-up every month INCREASE > 3 kg CONTINUE for 12 months DRUG WITHDRAWAL FURTHER TREATMENT according to expected benefit and obtained results Royal College of Physicians, 1998
Indications for surgical treatment • BMI > 40 kg/m2 • BMI 35 - 40 kg/m2depending on thethreat to life (National Health Institute of USA, 1991) Vertical gastric banding (VGB) Gastric by-pass operation
Factors influencing the outcome of obesity treatment • patient’s personality • motivation for treatment, satisfaction from treatment, realistic and individual goals • results of previous treatment attempts • class of obesity • the degree of health hazard, presence of obesity-related conditions