Download
1 / 40
460 likes | 1.77k Views
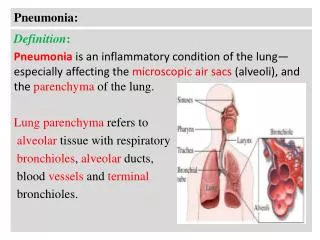
Pneumonia. Araya Satdhabudha , MD. Division of Pediatric Pulmonology & Critical Care Thammasat University. Epidemiology. Pneumonia is a common problem in children Particularly in children under 5 years Incidence 156 million children/year 95% in developing country

E N D
Pneumonia Araya Satdhabudha, MD. Division of Pediatric Pulmonology & Critical Care Thammasat University
Epidemiology • Pneumonia is a common problem in children • Particularly in children under 5 years • Incidence 156 million children/year • 95% in developing country • 7-13% faced with severe pneumonia • 0.29 episode/child-year in developing country • 0.05 episode/child-year in developed country • Pneumonia is the leading cause of death in developing country Bull World Health Organ 2008
Epidemiology and etiology of childhood pneumoniaWorld Health Organization Bulletin of the World Health Organization 2004
Epidemiology : developing countries In 1998 • 10 million of children < 5 yrs were died each year • 3 million child died from pneumonia (most from measles, pertussis) Recent data • Pneumonia still cause around 2 million children’s death annually • About 20% of all child death • 70% in Africa and Asia • Africa and Asia record 2-10 times more children with pneumonia than in USA Bull World Health Organ 2008
Epidemiology : Thailand • 45-50 % of LRTI in children under 5 years are diagnosis as pneumonia • Pneumonia is the leading cause of death in children under 5 years • 19% of fatal children are caused by pneumonia (2 million children/year) J Med Assoc Thai 2002 Lancet 2005
ข้อมูลจาก สำนักระบาดวิทยา กรมควบคุมโรค กระทรวงสาธารณสุข ปี 2548-2553
ข้อมูลจาก สำนักระบาดวิทยา กรมควบคุมโรค กระทรวงสาธารณสุข ปี 2548-2553
ข้อมูลจาก สำนักระบาดวิทยา กรมควบคุมโรค กระทรวงสาธารณสุข ปี 2548-2553
ข้อมูลจาก สำนักระบาดวิทยา กรมควบคุมโรค กระทรวงสาธารณสุข ปี 2548-2553
ข้อมูลจาก สำนักระบาดวิทยา กรมควบคุมโรค กระทรวงสาธารณสุข ปี 2546-2555
Risk factors • Low birth weight (premature, SGA) • 20% of children born in developing countries have birth weight under 2,500 gm. • Under- nutrition, hypovitaminosis A, Zinc def. • W/A Z score of <-2 to -3 had 2-3 higher risk of death due to ALRI (Am J Epidemilo 1996) • Lack of breastfeeding • Motality rate associated with both ALRI and diarrhoae was increased 6 times by not breastfeeding • Air pollution : • Household use of fuels • ETS : RR of 1.2 for ARI in maternal smoking (J Infect Dis 1988) • Overcrowding : day-care centers Paediatric Respiiratory reviews 2005
Etiology • 15-60% : cannot identify the pathogen • Age is a good predictor of the likely causative agent Kendig’s Disorders of Resp Tract in Children 2012 JID 2004 N Engl J Med 2002
Clinical evaluation Atypical pneumonia : may be no fever • Fever • Cough • Dyspnea May be absent in early stage of LRI • Tachypnea • Nasal flaring, Retractions, Chest indrawing • Grunting • Crepitation • Wheezing • : the most sensitive sign sensitivity 74% specificity 67% : impending respiratory failure : auscultation may not be present in early pneumonia Paediatric respiratory reviews 2000 Arch Dis child 2000
WHO’s age - specific criteria for tachypnea Age < 2 mo : RR > 60/min Age 2-12 mo : RR > 50/min Age 1 – 5 yrs : RR > 40/min Age > 5 yrs : RR > 30/min
Clinical clue for CAP • Daycare attendance :Viral infection, DRSP • Exposure to infectious diseases : Viral or Mycoplasma infection, Tb • Hospitalization : Nosocomial infection • Missing immunizations : H. influenzae, pertussis, measles • Antibiotic therapy within previous month : Infection with resistant bacterial strains • Recent travel : influenza, SARS
Investigations • blood culture in all hospitalized children but low blood culture yield (< 10%) J Infection 2004; 48: 134-8 • Blood culture in child with high fever or looked sepsis. • BTS guidelines for CAP in children.thorax 2011 NP aspirate for virus in all children aged < 18 months (highly specific and sensitive) J Infection 2004; 48: 134-8.
Investigation for CAP in children Am Fam Physician 2004; 70:899-908.
CXR • CXR may not be abnormal at the start of classical pneumonia • If all the physical signs of pneumonia are not present, CXR are unlikely to be helpful. • The child should be perform CXR, when • Age < 5 yrs without localizing sign • Complicated pneumonia : pleural effusion, atelectasis • Atypical presentation • Not respond to antibiotic with in 48-72 hr. BTS guideline for CAP pneumonia in children, Thorax 2011 Paediatric respratory review 2000
Suggestive features of bacterial LRI • clinical • Fever > 38.5○C • abrupt onset • dyspnea • crepitation • CXR • alveolar process, • lobar consolidation Kendig and Chernik’s disorders of the respiratory tract in children.2012.. Am Fam Physician 2004; 70:899-908.
Suggestive features of viral LRI • clinical • Infants and young children • fever < 38.5○C • gradual onset • dyspnea • crepitation, wheeze • CXR • Hyperinflation • interstitial process • patchy collapse (25%)
Suggestive features of mycoplasma LRI • CXR • Interstitial infiltrate, lobar consolidation and hilar adenopathy • clinical • School aged children • fever (30%), Cough(90%), rales (62%), wheeze /rhonchi(36%) • Extrapulmonary manifestation Kendig and Chernik’s disorders of the respiratory tract in children.2012.. BTS Guideline. Thorax 2011 Am Fam Physician 2004; 70:899-908.
Microbiological investigations : bacteria BTS guidelines for CAP in children.thorax 2011 J Infection 2004
Microbiological investigations : atypical pneumonia and virus BTS guidelines for CAP in children.thorax 2011 J Infection 2004.
Severity assessment BTS guidelines for CAP in children.thorax 2011
Indication for admission • Age < 3 months • Desaturation (SpO2 < 92% in roomair) • Dyspnea(increase WOB, retraction, grunting • Poor feeding or dehydration • Lethalgy or sign of shock : peripheral cyanosis, poor capillary refill • S.aureus pneumonia • Underlying disease: CHD, CLD, immune def. • Clinical not improve within 48 hr after Rx • Family not able to provide appropriate observation or supervision BTS guidelines for CAP in children.thorax 2011
Indications for PICU admission • Require FiO2 > 0.6 to maintain SpO2 > 92% • Shock • Sever respiratory distress, exhaustion (rising RR and PR ± ↑PaCO2) • Recurrent apnea • Slow, irregular breathing BTS guidelines for CAP in children.thorax 2011
General management At home • Supportive and symptomatic treatment for • Fever • cough • preventing dehydration : force oral fluid as tolerate • identifying any deterioration • The child should be reviewed by the doctor if • Deteriorating • not improved after 48 hrs of treatment BTS guidelines for CAP in children.thorax 2011
At hospital • Oxygen therapy: • In child with dyspnea, cyanosis, desaturation • maintain SpO2 > 92% • Fluid therapy : • Avoid nasogastric tube • Start iv fluid : mark dyspnea, abdominal distension, dehydration • Avoid volume overload, monitor serum electrolytes • Managing fever and pain • Bronchodilator inhaled : wheezing or rhonchi • Physiotherapy (no role in distress, acute pneumonia) • Frequent monitoring (vital signs, SpO2, lung signs, respiratory pattern BTS guidelines for CAP in children.thorax 2011
Specific treatment Clinical Practice Guideline for Treatment of Childhood Pneumonia in Thailand ชมรมโรคระบบหายใจและเวชบำบัดวิกฤตในเด็ก พ.ศ. 2555
Antiviral drug MMWR Jan 2011
Prevention • Promote adequate nutrition including breastfeeding and zinc intake • Raising immunization rate • Pneumococcal conjugated vaccine • Hib vaccine • Measles vaccine • Pertussis vaccine • Influenza vaccine • Reducing indoor pollution • Household use of fuels • Environmental tobacco smoke • Hand washing BTS guidelines for CAP in children.thorax 2011 Paediatric Respiratory Rewiews 2011