Download
1 / 31
350 likes | 745 Views
COMMON ANEMIAS. Haematology. Dr. Janis Bormanis. Common anemias. Iron deficiency Megaloblastic anemias Secondary anemias to chronic diseases Anemia of chronic disease Hemolytic anemias Spherocytic fragmentation. BODY IRON IN THE POPULATION. RELATIVE FREQUENCY. IDA. IDWA.

E N D
COMMON ANEMIAS Haematology Dr. Janis Bormanis
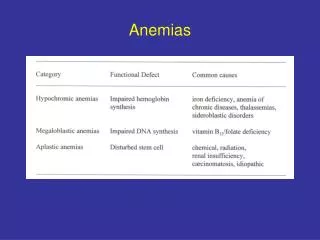
Common anemias • Iron deficiency • Megaloblastic anemias • Secondary anemias to chronic diseases Anemia of chronic disease • Hemolytic anemias Spherocytic fragmentation
BODY IRON IN THE POPULATION RELATIVE FREQUENCY IDA IDWA INC HC STR IRON DEFICIENCY OVERLOAD
STAGES OF IRON DEPLETION Loss of body stores Fall in serum iron Anemia develops Microcytosis Hypochromasia
ASSESSMENT OF IRON STATUS • Identify high risk groups • Children • Menstruation • Pregnancy - Lactation • Frequent Blood Donors • Chronic GI loss • Malabsorption • Diet
SOURCES OF IRON • Heme Iron • Meat • 10-15% absorbed • Non-Heme • Vegetables, Fruit, Cereal • Major source in Third World
IRON BALANCE • Ingest 10-20 mg. per day • Absorb 1-3 mg. per day • Lose 1 + mg per day • menstrual loss 30-50 ml • Total iron 35-50 mg/kg • Stores 1 gram • Easy to achieve negative balance
Dx of IRON DEFICIENCY • Symptoms and signs • CBC - Anemia - microcytosis - Hypochromia • Blood Film - Oval - pencil - Tear • Serum Fe and TIBC Fe low TIBC high • Serum Ferritin • Cause of Iron Deficiency
INVESTIGATION OF CAUSE • Investigate when cause not Clear • Symptoms of cause often unreliable • Upper GI cause higher Yield • If upper GI lesion found then a colonic lesion unlikely • TESTS - Radiologic, Endoscopic Biopsy, Angiographic.
THERAPY Replace iron
Anemia of Chronic disease • Usually mild to moderate anemia • normocytic normochromic • low retic count • Low serum Fe and low TIBC sat % 15-20 • Ferritin normal or high • A responsible disease is present • Usually a systemic disorder
Megaloblastic Anemias Vitamin B12 Folic Acid
Reasons for measuring B12 • Investigation of macrocytic anemia • Investigation of any anemia • Investigation of fatigue • Routine Geriatric Screen • Investigation of neurologic symptoms
Symptom Complex • Classic presentation uncommon • Often a screen in older patients • Memory loss prominent • Neuropathy • Changes in evoked potential • Non specific symptoms of anemia
Causes Pernicious anemia • 10 % of all cobalamin deficiencies • Majority are due to malabsorption
Causes of Low Serum B12 Malabsorption of free cobalamin • Pernicious anemia • Post gastrectomy state • Small bowel diseases
Causes of Low Serum B12 Malabsorption of food cobalamin • Atrophic gastritis • Postgastrectomy state • Chronic nonspecific gastritis (H pylori ?) • H2 receptor blocking agents
Tests • CBC - RBC indices • Most are macrocytic • Blood film • Macro-ovalocytes - hypersegmented polys • Biochemical abnormalities • LDH bilirubin • Serum B12 • Schilling test
Folic acid deficieny • Dietary source is vegetables • Absorption no specific carrier • Deficiency mainly dietary. • Alcoholism a risk • Anemia macrocytic • No neurologic symptoms • Measure RBC folate
Therapy Replace B12 - folic acid
Hemolytic anemias • History of jaundice and anemia • May have splenomegaly • May have a family history • anemia with reticulocytosis • specific morphologic changes • serum bilirubin and LDH as markers • Specific tests follow morphology
These are just some of the anemias which illustrate principles of diagnosis
Approach to anemia • Anemia is not a disease • There is usually a cause • investigation should be logical • Start with CBC and Blood film • Leads to other tests • non specific • specific • Guides therapy