Download
1 / 47
490 likes | 728 Views
Maternal Isoimmunisation. Maternal Isoimmunisation. MATERNAL ALLOIMMUNIZATION, ALSO KNOWN AS ISOIMMUNIZATION, OCCURS WHEN A WOMAN’S IMMUNE SYSTEM IS SENSITIZED TO FOREIGN ERYTHROCYTE SURFACE ANTIGENS, STIMULATING THE PRODUCTION OF IMMUNOGLOBULIN G (IGG) ANTIBODIES.

E N D
Maternal Isoimmunisation MATERNAL ALLOIMMUNIZATION, ALSO KNOWN AS ISOIMMUNIZATION, OCCURS WHEN A WOMAN’S IMMUNE SYSTEM IS SENSITIZED TO FOREIGN ERYTHROCYTE SURFACE ANTIGENS, STIMULATING THE PRODUCTION OF IMMUNOGLOBULIN G (IGG) ANTIBODIES
Causes of Maternal Isoimmunisation. • Causes of Rh Isoimmunisation • Biochemistery of Rh Antigen • Genetic of Rh Antigen. • Mechanis of Rh Isoimmunisation • Pathogeneisis of Fetal Rh Diseaes. • History Management of Rh Disease. • Prevention of Rh Isoimmunisation. • Treatement of cases of Rh isoimmunisation. • Other cases of meternal Isoimmunisation
Maternal Isoimmunisation Among the antigens capable of causing maternal alloimm- unization and fetal hemolytic disease, the Rh blood group system is the most common. In particular, the D antigen of the Rh blood group system (Rh D) causes the most cases of severe hemolytic disease. • Because anti-D Ig prophylaxis has reduced the risk of sensitization to less than 1% of susceptible pregnancies, other alloantibodies have increased in relative importance. These include: • antibodies to other antigens of the Rh blood group system (c, C, e, and E), • -as well as other atypical antigens known to cause severe anemia, such as anti-Kell (K, k), anti-Duffy (Fya), and anti-Kidd (Jka, Jkb).
Causes of Maternal Isoimmunisation. • Biochemsitery and Genetic Rh Antigen. • Causes of Rh Isoimmunisation. • Mechanis of Rh Isoimmunisation • Pathogeneisis of Fetal Rh Diseaes. • History Management of Rh Disease. • Prevention of Rh Isoimmunisation. • Treatement of cases of Rh isoimmunisation. • Other cases of meternal Isoimmunisation
Rh-Isoimmunization- Biochemical Aspect of Rh Antigen The Rh antigen is a complex of three components: C, D, and E antigen. It is distributed on the cell membrane in a non-random fashion. Two of these antigens (C and E) have alleles that can be identified immunologically (by antisera). The third one (D) antigen has no antigenic allele I.e. no specific antisera for a “d” antigen. The presence of “D” antigen implies an Rh-positive blood.
Rh-Isoimmunisation- Genetics of Rh Antigen RH antigen is a genetically determined protein produced during Red Cells formation. It appears as early as the 38 days after fertilization. The Rh “gene complex” reside on the distal end of the short arm of chromosome one. Three genetic loci, each with two possible alleles determine the Rh antigen (Rh blood group)
Phenotype Genotype eCd/EcD D positive • Antigenicity of the Rh surface protein: • genetic expression of the D allele. • Number of specific Rh antigen sites. • Interaction of components of the Rh gene complex. • Exposure of the D antigen on the surface of the red cell e C d E c D
Race/Ethnicity Frequency (%) Caucasian 15-16 African American 8 African 4 Basque* 30-35 Asian <1 Asian American 1 Native American/Inuit 1-2 Eurasian 2-4 Rates of Rh Negativity Among Ethnic Groups • *Region of France/Spain
GeneComplex Frequency(%) CDe 41 c(d)e 39 cDE 16 cDe 2.2 C(d)e 1.1 c(d)E 0.6 CDE 0.08 C(d)E 0.00 Table 2. Rh Gene Frequencies in 2000 Unrelated Caucasian Adults The D antigen is the most immunogenic. Three pairs of Rh antigens exist with varying gene frequencies and possible combinations
Causes of Maternal Isoimmunization. • Genetic and Biochemistry of Rh Antigen. • Natural History of Rh Isoimmunization • Causes of Rh Isoimmunization. • Mechanism of Rh Isoimmunization • Pathogenesis of Fetal Rh Disease. • History Management of Rh Disease. • Prevention of Rh Isoimmunization. • Treatment of cases of Rh isoimmunization. • Other cases of maternal Isoimmunization
Natural History of Rh-Isoimmunization: If no preventive measures are taken: 0.7-1.8% of Rh negative women will become isoimmunized antenatally, developing D antibody through exposure to fetal blood. 8-17% will become isoimmunized at delivery. 3-6% after spontaneous or elective abortion. 2-5% after amniocentesis. In subsequent D-positive pregnancies of isoimmunized women, maternal D antibody will cross the placenta into the fetal circulation and hemolyze red cells.
Without treatment: 25-30% of the offspring will have some degree of hemolytic anemia and hyperbilirubinemia. 20-25% will be hydropic and often will die either in utero or in the neonatal period. Cases of hemolysis in the newborn that do not result in fetal hydrops still can lead to kernicterus.
kernicterus Is a neurological condition observed in infants with severe hyperbilirubinemia and is due to the deposition of un-conjugated bilirubin in the brain. • Causes of Neonatal Hyperbilirubinemia: • Excessive destruction of RBCs. • In the absence of placental clearance. • And immature ability of conjugating fetal bilirubin. Clinical Features of Kernicterus: Symptoms that manifest several days after delivery include poor feeding, inactivity, loss of the Moro reflex, a bulging fontanelle, and seizures. The 10% of infants who survive may develop spastic choreoathetosis, deafness, and mental retardation.
Causes of Maternal Isoimmunisation. • Genetic and Biochemistery of Rh Antigen. • Natural History of Rh Isoimmunisaton. • Factors that deterimine development of Rh Isommunisation • Causes of Rh Isoimmunisation. • Mechanis of Rh Isoimmunisation • Pathogeneisis of Fetal Rh Diseaes. • History Management of Rh Disease. • Prevention of Rh Isoimmunisation. • Treatement of cases of Rh isoimmunisation. • Other cases of meternal Isoimmunisation
Approximately 10% of Caucasian pregnancies are Rh incompatible. • However less than 20% of Rh D incompatible pregnancies • actually lead to maternal alloimmunization. In addition as many • as 30% of Rh D-negative individuals have been demonstrated • to not become alloimmunized even when challenged with • large volumes of Rh D-positive blood • Factors that affect the risk of development of alloimmunization • in a susceptible Rh D-negative woman: • volume of fetomaternal hemorrhage. • degree of maternal immune response (related to antigenicity of fetal RBCs and type of IgG) • concurrent ABO incompatibility
The Risk of development of Fetal Rh-diseaes is affected by: • The Risk of development of Maternal isoimmunisation: • - the husband phenotype and genotype ( 40 % of Rh positive men are homozygous and 60% are heterozygous). • - The antigen load and frequency of exposure. • - The classe of IgG. • - ABO incompatibility • The Extend of Severity of Fetal Hemolytic Diseases: • - Degree of expression of genetic expression of the D allele. • - Number of specific Rh antigen sites. • - Interaction of other components of the Rh gene compelex. • - Degree of exposure of the D antigen on the surface of the red cell Less than 20% of Rh D incompatible pregnancies actually lead to maternal alloimmunization
Role of ABO blood group status: • With an ABO-compatible fetus, the overall risk of alloimmunization if not treated with anti-D Ig is approximately 16%. However, if ABO incompatibility exists, the risk is only 1.5-2%. The protective effect conferred by ABO incompatibility is believed to be due to maternal destruction and subsequent clearance of the ABO-incompatible fetal erythrocytes before Rh sensitization can occur. • Role of Volume of Fetomaternal Hemorrhage: • Fifteen to 50% of births produce hemorrhage volumes sufficient to cause alloimmunization (as little as 0.1 mL and in rare cases can exceed 30 mL) depending on the maternal immune response
Causes of maternal alloimmunization • Blood transfusion • Fetomaternal hemorrhage • Antepartum • Intrapartum • Abortion • Therapeutic • Spontaneous • Ectopic pregnancy • Abruption • Abdominal trauma • Obstetric procedures • Amniocentesis • Chorionic villus sampling (CVS) • Percutaneous umbilical blood sampling (PUBS) • External cephalic version (ECV) • Manual removal of the placenta
Normal Pregnancy Risk TPH First Trimester 6.7 % Second Trimester 15.9 % Third Trimester 28.9 % Parturition 50 % Spontaneous Abortion 2 % Therapeutic Abortion 4 – 5 % Amniocentesis 15- 25 % Estimated Risk of Transplacental fetomaternal hemorrhage In most cases FM hemorrhage is around 0.1 ml. The amount necessary to cause Isoimmunisation is not known.
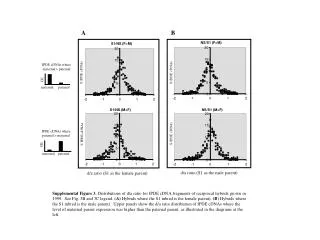
Fetomaternal hemorrhages occurs in as many as 75% of pregn- ancies. Its incidence increases as gestation advances and most cases occurs during delivery. Tests for detection and estimation of fetal blood in maternal circulation • Rosette screening test: is used to determine the presence of a fetomaternal hemorrhage. • The Kleihauer-Betke test: is employed to quantify the volume of hemorrhage so that an appropriate dose of anti-D Ig can be administered. • FlowCytometery:
Causes of Maternal Isoimmunisation. • Genetic and Biochemistery of Rh Antigen. • Natural History of Rh Isoimmunisaton. • Factors that deterimine development of Rh Isommunisation • Causes of Rh Isoimmunisation. • Mechanis of Rh Isoimmunisation • Pathogeneisis of Fetal Rh Diseaes. • History Management of Rh Disease. • Prevention of Rh Isoimmunisation. • Treatement of cases of Rh isoimmunisation. • Other cases of meternal Isoimmunisation
Mother 1. Cleared by Macrophage Primary Response 2. Plasma stem cells • 6 wks to 6 M. • IGM. IGM antibodies Placental Fetal Anaemia
Mother Macroph. antigen Presenting cell T- helper cell Seocndary Response • Small amount • Rapid • IgG B cell IgG Anti - D Placental Fetal Anaemia
Mother Macroph. Antigen Presenting Cell Group “O” Rh Negative T-Hellper Anti - A Anti - B B-cell Anti-D Placenta A Rh positive B Rh Positive Infant “O” Rh positive
Causes of Maternal Isoimmunisation. • Genetic and Biochemistery of Rh Antigen. • Natural History of Rh Isoimmunisaton. • Factors that deterimine development of Rh Isommunisation • Causes of Rh Isoimmunisation. • Mechanis of Rh Isoimmunisation • Pathogeneisis of Fetal Rh Diseaes. • History Management of Rh Disease. • Prevention of Rh Isoimmunisation. • Treatement of cases of Rh isoimmunisation. • Other cases of meternal Isoimmunisation
Prevention of Maternal Alloimmunisation: Exogenous administration of a dose of anti-D Ig sufficient enough to suppress an immune response, is known as antibody mediated immune suppression (AMIS). The mechanism of AMIS: the most likely mechanism is via central inhibition, wherein Rh Ig coats fetal erythrocytes, which are then sequestered in the spleen and lymph nodes. The local increase in antigen-antibody complexes interrupts the commitment of B cells to plasma cell clones, thereby suppressing the primary immune response. Additionally, these antigen-antibody complexes stimulate the release of cytokines by immune effector cells that inhibit the proliferation of antigen-specific B cells
Because fetal Rh antigens are present as early as the 30th day after conception, anti-D Ig is indicated with ectopic pregnancy as well as therapeutic and spontaneous abortions. The risk of alloimmunization in susceptible women undergoing therapeutic or spontaneous abortion is 4–5% and 1.5–2%, respectively. For pregnancies less than or equal to 12 weeks’ gestation, 50 mcg of anti-D Ig sometimes is administered because the entire blood volume of the fetus usually is less than 5 mL. However, pregnancies exceeding 12 weeks’ gestation or pregnancies in which gestational age is unknown should receive the full 300-mcg dose
Dose of prophylactic Anti-D Ig: 10 mcg of anti-D Ig should be administered for every mL of fetal blood in the maternal circulation. Thus, the 300-mcg dose is more than adequate for a typical feto- maternal hem- orrhage and covers hemorrhage volumes up to 30 mL of whole fetal blood. In the less than 1% of cases where the volume of fetomaternal hemorrhage exceeds 30 mL, utilizing the Kleihauer-Betke test to quantitate the volume of fetomaternal hemo- rrhage and admini- stering the appropriate amount of anti-D Ig (10 mcg/mL fetal blood) is necessary
Causes of Maternal Isoimmunisation. • Genetic and Biochemistery of Rh Antigen. • Natural History of Rh Isoimmunisaton. • Factors that deterimine development of Rh Isommunisation • Causes of Rh Isoimmunisation. • Mechanis of Rh Isoimmunisation • Pathogeneisis of Fetal Rh Diseaes. • History Management of Rh Disease. • Prevention of Rh Isoimmunisation. • Treatement of cases of Rh isoimmunisation. • Other cases of meternal Isoimmunisation
Management of cases of Rh isoimmunisation The goals in managing the alloimmunized pregnancy are 2-fold: Initially detecting fetal anemia prior to the occurrence of fetal compromise. Minimize fetal morbidity and mortality by correcting this anemia until fetal lung maturity and delivery can be achieved.
Past Obstetric History: Although not reliably accurate in predicting severity of fetal disease, past obstetrical history can be somewhat prognostic
Antibody Titer in maternal blood Titers greater than 1:4 should be considered Rh alloimmunized. However, the threshold for invasive fetal testing varies at different institutions and generally is 1:16 or greater because these titers have been associated with fetal hydrops
spectrophotometric measurements of bilirubin in amniotic fluid Because the wavelength at which bilirubin absorbs light is 420-460 nm, the amount of shift in optical density from linearity at 450 nm (D OD 450) in serial amniotic fluid samples can be used to estimate the degree of fetal hemolysis. Modification of the Liley curve to adjust for the relative inaccuracy of D OD 450 readings in early-to-middle second trimester and the use of serial measurements has improved its accuracy.
Fetal Blood Sampling The only definitive means of diagnosing fetal anemia and acidosis is via fetal PUBS, also known as cordocentesis Despite the wealth of information afforded by PUBS, routine umbilical cord blood sampling is not universal due to concern for fetal and maternal complications. These include fetomaternal hemorrhage, fetal loss (0.5–2% per procedure), placental abruption, acute refractory fetal distress, and amnionitis with maternal adult respiratory distress syndrome.
the role of ultrasound Ultrasound is primarily used to assess fetal well being; diagnose hydrops; and guide amniocenteses, fetal blood sampling, and IUTs. In this capacity, ultrasonography has improved both the safety and success rate of invasive procedures, as well as helping to minimize invasive testing.
Doppler blood flow measurment: Doppler studies have not been successful in demonstrating accurate prediction of fetal anemia. Mari et al, 2000, purport that increases in peak velocity of systolic blood flow in the middle cerebral artery can be used to detect moderate and severe anemia in nonhydropic fetuses. However, it does not identify milder cases of anemia consistently, and results should therefore be interpreted with caution. Doppler flow studies ultimately may be quite useful for cases of non-D alloimmunization, such as those observed with the Kell antigen, because in these patients the degree of fetal anemia correlates poorly with the extent of erythrocyte destruction and the D OD 450, rendering amniotic fluid studies ineffective
considerations for PUBS and possible IUT A number of important considerations exist when preparing a patient for PUBS and possible IUT; these include: gestational age, possibility of delivery, fetal maturation with corticosteroids, and likelihood of transfusion The amount to be transfused can be calculated once the hematocrit/hemoglobin results are returned. In general, 30-60 mL/kg of nonhydropic fetal weight is transfused
Current Indication of IPT In the setting where repeat access cannot be gained or with a posterior placenta in which intravascular access could not be gained initially, performing an IPT is reasonable. IPT require a greater volume of blood, roughly calculated as the following: (# of weeks’ gestation – 20) x 10 mL Care should be taken to avoid the umbilical vessels and to ensure that intraabdominal access is indeed intraperitoneal.
IVT vs. IUT Benefits of IVT over IPT include: Direct measurement of the fetal hemoglobin and acid-base status. Lower failure rate (particularly in the hydropic fetus). Lower rates of procedure-related morbidity and mortality. Better efficacy at earlier gestational ages. The only benefit offered by IPT is the ability to drain off fetal ascites during the procedure, but this is of minimal benefit in a hydropic fetus
Causes of Maternal Isoimmunisation. • Genetic and Biochemistery of Rh Antigen. • Natural History of Rh Isoimmunisaton. • Factors that deterimine development of Rh Isommunisation • Causes of Rh Isoimmunisation. • Mechanis of Rh Isoimmunisation • Pathogeneisis of Fetal Rh Diseaes. • History Management of Rh Disease. • Prevention of Rh Isoimmunisation. • Treatement of cases of Rh isoimmunisation. • Meternal Isoimmunisation to Rare antibodies.
Maternal Isoimmunisation to rare antibodies Patients with serum antibody known to cause hemolysis in the fetus, such as anti-c, anti-Kell and anti-E antibodies, these patients are managed similarly to the patient who is Rh sensitized. Initial management involves following serial maternal antibody titers, which leads to assessment of the fetus for hemolysis using amniocentesis as indicated by rising antibody titers, ultrasound, and possibly PUBS.
Disease Frequency • Antibodies • Common • Kell, c, E • Uncommon • e, C, cE, Ce, Cw, Kpa, Kpb, k, Jka, s, Wra, Fya • Rare • Biles, Coa, Dia, Dib, Doa, Ena, Fyb, Good, Heibel, Jkb, Lua, Lub, M, Mia, Mta, N, Radin, S, U, Yta, Zd • No documented cases • Lea, Leb, P • Table 3. Association of Atypical Erythrocyte Antibodies and Hemolytic Disease of the Newborn
Two situations exist in which patients are not followed identically to patients who are Rh sensitized. The first is that of alloimmunization to the c, E, or C antigens. Some concern exists that hemolysis may occur in these patients with a lower than 1:16 titer. Thus, if the initial titer is 1:4 and stable but increases at 26 weeks’ gestation to 1:8, assessing with amniocentesis for D OD 450 at that point is reasonable. If, however, the patient presents in the first trimester with a 1:8 titer that remains stable at 1:8 throughout the second trimester, continued serial antibody titers are indicated
The second case in which patients should not be managed identically to patients who are Rh sensitized is that of Kell isoimmunization because several cases of severe fetal hemolysis with anti-Kell antibodies have occurred in the setting of low D OD 450 values. The proposed etiology for this is that the anti-Kell antibodies may attack and destroy erythroid precursors that have low levels of hemoglobin. This leads to fetal anemia but not with the concomitant rise in bilirubin breakdown products, thus leading to relatively normal values of the D OD 450.
This type of ABO incompatibility also can lead to mild fetal hemolysis. Because most of the anti-A and anti-B antibodies are immunoglobulin M (IgM), which does not cross the placenta, the fetal hemolysis does not lead to severe anemia and hydrops. However, even with mild anemia, the hemolysis may lead to hyperbilirubinemia and even kernicterus, thus closely monitor these patients postpartum for jaundice. No particular antepartum management needs to be addressed in the setting of ABO incompatibility.