Download
1 / 35
350 likes | 490 Views
IV Therapy. Sue Bouma RN BSN CRNI. • Right Patient: treat as any drug, use MAR for accuracy in administration • Right Drug: solution for IVs, inspect prior to hanging • Right Dose: consider w/time, Amount of IV solution to hang • Right Time: rate of solution administration

E N D
IV Therapy Sue Bouma RN BSN CRNI
• Right Patient: treat as any drug, use MAR for accuracy in administration • Right Drug: solution for IVs, inspect prior to hanging • Right Dose: consider w/time, Amount of IV solution to hang • Right Time: rate of solution administration • Right Route: specific order for IV admin • Right Documentation: Always
What are the two most important aspects of IV therapy? • Six rights of medication administration • Patent line • First do no harm
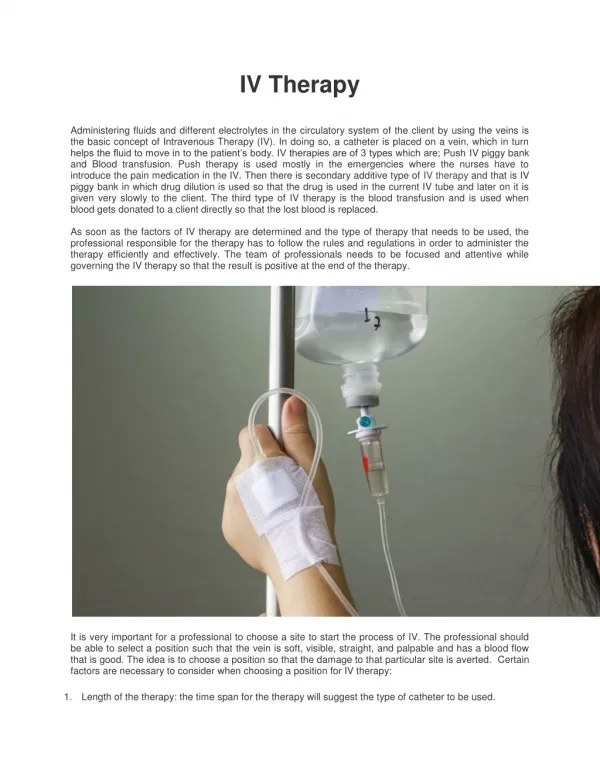
What is extravasation? Extravasation is the accidental administration of intravenously (IV) infused medicinal drugs into the surrounding tissue, either by leakage (e.g. because of brittle veins in very elderly patients), or direct exposure (e.g. because the needle has punctured the vein and the infusion goes directly into the arm tissue). Extravasation of medicinal drugs during intravenous therapy is a side-effect that can and should be avoided
What is infiltration? • Infiltration is the diffusion or accumulation (in a tissue or cells) of substances not normal to it or in amounts in excess of the normal
Septicemia • Severe blood infection, may result from contamination externally or internally from any venous access device.
Anaphylactic Reaction • Severe allergic reaction. • What are the symptoms?
Speed shock • Too much too fast. • Manifest as drug toxicity or possibly fluid overload. • Patient would not have reacted if amount or dosage would have been within a normal range.
Circulatory overload • Too much fluid for body to assimilate, not necessarily tied to speed of delivery, but may be. • Think RBC’s being given to an older adult, what could happen?
Air Emobolism • Can result in death. • More common with CVAD’s, accidental or improper removal of device. • How do you treat it?
Hematoma • A collection of blood outside of the blood vessels. • No discontinuing arterial lines or sheaths. • How long do I keep pressure on a peripheral IV or central line I have dcd?
Phlebitis • Inflammation of the vein
Thrombophlebitis • Inflammation of the vein with thrombus formation. • What are the symptoms? • May need doppler study with CVAD to correctly diagnose.
Infection • This refers to infection at the site of the IV or CVAD. • What are the symptoms? • Needs rx with antibiotics so infection does not become systemic.
CVAD • PICC-many on the market. • Know what kind of PICC you are working with. • Solo • Groshong • Power PICC How do you know your line is central? What do I do if the patient comes from another hospital with a PICC?
Care of PICC lines • Institution should have care of these lines in their PP. • ALWAYS use a 10cc syringe to flush. • What do I do if I believe the PICC line has migrated out? • I have a 3 lumen PICC line, but 2 of the lumens are clotted and do not work, but that’s ok, I only need 1 port! Is this ok?
What about HIT? • Heparin induced thrombocytopenia.
Hickman catheters • Always requires a heparin flush. • Should always get a blood return.
Subclavian and Swan Ganz lines • Fallen out of favor. • May still be used on CABG patient. • SG measures PAP,CVP, PAWP, CO, cardiac index, and usually temperature. • SC approach considered dirtiest area to have a CVAD.
Implanted portacaths • Always a heparin flush • Should always get a blood return. • Need training to access. • You will not be accessing these in clinical. • What do I do if there is no blood return? • Power and nonpower, need a power huber needle to inject on power ports.
Perma-cath • Used for dialysis or plasmapheresis. • Not as common as other CVADs.
How do I decide what kind of access my patient need? • Doesn’t the doctor know? • Are they the ones making the decision?
Are there any ethical concerns in IV therapy? • What do you think?