Download
1 / 77
880 likes | 1.62k Views
Trematodes (Flukes) and Cestodes. Jose A. Serpa, M.D. Assistant Professor Baylor College of Medicine. References. The Travel and Tropical Medicine Manual by Elaine Jong and Christopher Sandford. Fourth Edition, 2008

E N D
Trematodes (Flukes) and Cestodes Jose A. Serpa, M.D. Assistant Professor Baylor College of Medicine
References • The Travel and Tropical Medicine Manual by Elaine Jong and Christopher Sandford. Fourth Edition, 2008 • Principles and Practices of Infectious Diseases. Mandel, Bennett and Dolin. Sixth Edition, 2005 • DPDx. Laboratory Identification of Parasites of Public Health Concern (CDC). Second Edition, 2006. • Special thanks to Dr. A.C. White Jr. for allowing me to use some of his slides
Agenda • Trematodes (flukes): definition and classification • Schistosomes, liver flukes and lung flukes • Cestodes: Intestinal tapeworms • Cestodes: Tissue (cyst) stage (cysticercosis and ecchinococcosis)
Cayetano Heredia National Hospital and Institute of Tropical Medicine Alexander von Humboldt, Lima , Peru
Trematodes The flukes, or trematodes, are leaf-shaped parasites with a blind bifurcate intestinal tract Size varies from 1 mm to more than 10cm Most are hermaphroditic, except schistosomes
Classification • Blood flukes (Schistosomes) • Hepatobiliary (Clonorchis sinensis, Opistorchis spp. and Fasciola hepatica) • Lung flukes (Paragonimus) • Intestinal flukes (Metagonymus, Heterophyes, Fasciolopsis)
Eggs of trematodes From DPDx, website for laboratory diagnosis of parasitic diseases of the Division of Parasitic Diseases, National Centers for Infectious Diseases, Centers for Disease Control and Prevention, Atlanta, GA, [http://www.dpd.cdc.gov/DPDx/].
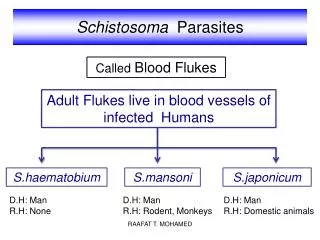
Schistosomiasis • Trematode infection caused by “blood flukes” which live in venules of the gastrointestinal and genitourinary tract • There are approximately 200 million persons infected in the world (120 million are symptomatic and 100 000 die each year) • It affects 74 countries (80% of cases occur in Sub-Saharan Africa)
Human Schistosomes and their geographic distribution S. mansoni:Africa, Brazil, Middle East, Caribean S. haematobium:Africa, Middle East S. japonicum: China, Phillipines, SE Asia S. mekongi: Laos, Cambodia S. intercalatum: Central Africa (less common)
Life cycle Cercariae penetrate human skin during contact or immersion in fresh water inhabited by infected snails Cercariae transform into schistosomulae , go into bloodstream and then migrate to liver and lung where they mature (4-6 weeks) Adult male and female pair and migrate to the Sup Mes vein (S. japonicum and S. mekongi), Inf Mesenteric vein (S. mansoni) or venous plexus sorrounding the bladder (S. hematobium) Eggs are excreted in feces or urine and deposited in fresh water. They hatch, miracidia emerge and infect snails of certain species. Cercariae emerge from infected snails
Clinical syndromes • Asymptomatic • Schistosome (cercarial) dermatitis • Acute Schistosomiasis • Chronic Schistomiasis
Schistosome dermatitis It is due to skin penetration of cercaria Pruritic maculopapular rash It can last from hours (first time exposed) to days (previously sensitized)
Acute Schistosomiasis (Katayama fever) • Occurs at the time of initial parasite egg-laying (hypersensitivity to egg- associated Ags) about 2-8 weeks after infection • Consists of fever, rash/urticaria, cough, abdominal pain, diarrhea, hepatosplenomegaly and eosinophilia • Usually in persons from non-endemic areas • More common with S. mansoni and S. haematobium
Chronic Schistosomiasis • Intermittent dysentery and bowel obstruction • Hepatosplenic disease • Urinary tract disease • Less common: Lung or CNS disease
Hepatosplenic schistosomiasis Occurs in S. mansoni , S. japonicum and S. mekongi Pathogenesis: granulomas around embolized eggs that become trapped in small portal veins (liver) Initial stage: hepatomegaly Later stages: Periportal fibrosis blocks portal blood flow which leads to portal hypertension (splenic congestion, ascites and esophageal bleed) HBV or HCV coinfection worsens prognosis
Urinary tract disease Occurs in S. haematobium infections Passage of eggs through the bladder wall cause hematuria and dysuria (inflammation and ulcerations) Granulomatous lesions with subsequent fibrosis of the bladder wall cause urinary reflux and obstruction (hydroureter, hydronephrosis, chronic bacteriuria, renal failure and squamous carcinoma of bladder)
Lung and CNS schistosomiasis • Eosinophilic pneumonitis results when eggs reaching the general circulation are trapped in the alveolar capillaries • Aberrant migration of adult worms or embolization of eggs to the spinal cord or brain can cause transverse myelitis (S. mansoni or S. haematobium) or seizures (S. japonicum) respectively
Keep in mind… • Acute infection of humans with avian species of Schistosomes can result in an allergic skin reaction called swimmer’s itch (can not mature in the human host and die in the skin). NO need of antiparasitic therapy • Pathogenic adult Schistosoma can persist in the human host for decades so infections can present in non endemic areas among immigrants from endemic regions
An interesting association • Prolonged and recurrent Salmonella bacteremia and/or bacteriuria has been reported in patients chronically infected with schistosomiasis
Diagnosis • Persons with a history of freshwater exposure in endemic areas (even if eosinophilia is absent) • Identification of eggs in stool or urine samples • Identification of eggs in tissues (e.g. rectal or bladder mucosa) • Serologic tests (CDC): FAST-ELISA (99% sensitive) and immunoblot (species-specific) • Imaging studies (US, CT, MRI) as clinically indicated
Treatment • Praziquantel is the drug of choice • Dosing: 40mg/kg in 2 divided doses on a single day (S. mansoni and S. haematobium) or 60mg/kg in 3 divided doses 4-6h apart on a single day (S. Japonicum) • Artemisinins (e.g. artemether) has antischistosomal as well as antimalarial activity • Steroids can be used along with praziquantel for Katayama fever or CNS disease
Prevention and control of Schistosomiasis • Avoid contact with fresh water in endemic areas • Annual mass drug administration of praziquantel • Environmental measures to control the snails and promote sanitary disposal of human excrement (cost beyond the reach of poor countries)
Liver flukes • They include: • Clonorchis sinensis • Opisthorchis sp. • Fasciola hepatica
Clonorchis and Opisthorchis Largely found in the Far East, Southeast Asia and Russia The hermaphroditic adult worms measure 5 to 25mm x 2 to 5mm and inhabit the intrahepatic biliary ducts Humans become infected by eating raw or inadequately cooked fish
Clinical syndromes • Asymptomatic eosinophilia • RUQ abdominal pain with jaundice • Acute biliary obstruction • Acute pancreatitis • Recurrent pyogenic cholangitis • Cholangiocarcinoma
Diagnosis and Treatment Based on identification of eggs in the stool or adult worms during surgery or ERCP Imaging studies (US, CT or MRI) can demonstrate biliary dilation Praziquantel is the drug of choice (75mg/kg in 3 divided doses 4-6h apart). Surgery or ERCP for acute biliary obstruction
Fasciola hepatica Large liver fluke (adult worm measures 3.0 x 1.5 cm) that lives in the bile ducts of its mammalian hosts (humans, sheep and cattle) Reported in 61 countries from Europe, North Africa, Asia and South America (Bolivia and Peru) More than 3 million cases in the world
Transmission Parasite eggs passed in stools hatch into miracidia which infects fresh water snails. Cercaria emerge from snails and attach to aquatic plants (encyst as metacercaria) Humans ingest contaminated aquatic plants (e.g. water cress) Metacercaria excyst, penetrate the intestinal wall, enter the peritoneum, and then pass through the liver capsule to the biliary tract
Clinical syndromes • Acute phase • Associated with parasite migration (duodenum – peritoneal cavity – liver) and burrowing through the liver • Causes fever, abdominal pain, hepatomegaly and eosinophilia 2. Chronic phase • Due to biliary involvement • Intermittent “biliary colic”, cholangitis
Diagnosis and management • Serology for acute phase • Demonstration of eggs in stools, bile or duodenal aspirates • Imaging studies (US, CT) show linear hepatic tracts • Treatment is with triclabendazole (10mg/kg once or twice). Also bithionol, nitazoxanide.
Lung flukes Most important species: Paragonimus westermani, P. heterotremus, P. skrjabini, P. miyazakii (Asia),P. africanus, P uterobilateralis (Africa), P. mexicana, P ecuadoriensis (South and Central America) Cases reported from Asia, Africa and Central and South America
Life cycle Adult worms lay eggs that are coughed up in the sputum or swallow and passed in the stools Eggs hatch in freshwater and develop into miracidia that infects snails (cercaria) Cercaria infects freshwater crustaceans (metacercaria) Humans are infected when eating raw or inadequately cooked crabs or crayfish Metacercaria excyst in the duodenum peritoneum diaphragm pleura lung
Clinical manifestations • Pulmonary paragonimiasis • Extrapulmonary paragonimiasis
Pulmonary paragonimiasis • Resembles pulmonary tuberculosis • Initial stages: cough productive of brownish sputum with intermittent hemoptysis • Chronic stages: profuse expectoration, dyspnea, hemoptysis, pleural effusions and pneumothorax • CRX: infiltrates, cavities, cysts, nodules, pleural effusions
Extrapulmonary paragonimiasis • Ectopic migration of eggs from the bowel • Most common: CNS, skin, liver, peritoneum • CNS: brain lesions (seizures, headaches, visual disturbances), meningitis • Skin: Migratory lesions (resemble cutaneous larva migrans)
Diagnosis and treatment • Identification of eggs in stools or sputum • Gram or AFB stain in sputum may destroy eggs • Serology: Immunoblot from CDC (Sen: 96%, Sp: 100%) • Drug of choice is praziquantel (75mg/kg/day divided in 3 doses for 2 days)
Tapeworms (adult stage) • Tapeworms are segmented flat worms that have a head or scolex (which attaches to the intestine) and rhomboid-shaped segments termed proglottids • The tapeworms elongates from each scolex by forming proglottids (which contain male and female reproductive organs). Adult tapeworms may reach lengths of 4.5 – 10m
Life cycle: generalities • The proglottids (containing eggs) shed periodically in the feces • Eggs are ingested by an intermediate host - cow, pig, fish. Then the eggs hatch and larvae emerge, penetrate the gut and migrate to the tissues (especially the muscle) • The lifecycle is completed when humans ingest encysted larvae-containing meat
Epidemiology • T. solium is prevalent worldwide (60 million) but rare in US except in immigrants from endemic areas of Latin America and Asia • T. saginata is found worldwide (60 million), especially in Africa and Latin America. In the US, it is seen among people who eat raw or undercooked beef (e.g. steak tartare) • D. latum is prevalent worldwide (10 million) particularly among people who ingest raw, pickled, or marinated fish. D. latum in the US has been associated with sushi and sashimi made of raw pacific salmon and some Scandinavian pickled fish dishes (carp, herring, smelt) • H. nana and H. diminuta(dwarf, 2cm long) is prevalent worldwide (30 million) especially in children. Because of person to person spread, nurseries and day-care facilities are sites of transmission