Download
1 / 69
690 likes | 705 Views
This report examines the incidence, risk factors, stage at diagnosis, treatment, survival, and mortality of lung cancer. It also explores the need for screening and early diagnosis, as well as addressing health inequalities. The report provides key messages and limited recommendations.

E N D
Cancer – Health Needs Assessmentoverview and focus on Lung Greg.fell@bradford.nhs.uk To contents
Approach to presentation • This IS the report. There is no accompanying document. • Additional notes are contained within the notes pages beneath each slide. • File......print.....notes pages.....
Approach to data • No new data analysis. • Revised and pulled together what exists already. • NYCRIS – QAd and high quality data set – as good as there is. • A little old (but reflects QA). • We hold local data, but: • QA / analyst capacity / ability to pull it ALL together. • Sub regional data has major issues in terms of statistical reliability and robustness. • Is Bradford different to any other multi ethnic population? • Other (mostly older) analyses done. • Have findings of these been implemented? • Has the epi changed since then? Probably not. • Populations, demographics, social characteristics, risk profile changes very slowly. • No major innovations in Rx? • Thus a new analysis might not give significant new conclusions – and will incur and OC in terms of analyst time. • Conclusions that can already be drawn from this. What are we measuring • Incidence – a measure of risk factor distribution • Stage at presentation – a measure of the efficiency of pick up by health care, broader social and cultural factors • Mortality – a measure of effectiveness of treatment and incidence • Survival – a measure of treatment effectiveness, and is also influenced by stage of Dx To contents
Questions and issues explored • Equality – best and worst. • Most common cancer diagnoses • Incidence • A reflection on exposure to risk factors • Survival gap? • Survival being a key measure of effectiveness of treatment once diagnosed. • Late Dx? Staging or mets at presentation. • Mortality • A refection of incidcne and treatment effectiveness. • What does the QOF tell us? – • Not much!!! Prev of all Ca. Might be possible to age standardise to take into account practice differences. • What can be done re stage at presentation – Sx awareness? • Dimensions of equality - Socio economic, ethnic. To contents
Contents • Summary / key messages. If you read nothing else read this. • Populations • Common Risk Factors • Screening • Overview of all Cancers • Lung Cancer • Risk Factors • Incidence • Stage at Diagnosis • Treatment • Survival • Mortality • Summary To contents
Summary This section summarises the key issues, limited recommendations. Discussion with CLAN re exactly what next is needed. To contents
Summary (1) – Risk Factors and populations • Significant variation across groups. Smoking and other risk factors. • Under implementation of preventive interventions – both in clinical practice and broader public health. • Not just smoking, though this is very important. • Opportunities for smoking cessation referral (especially at key life points – receptive to change. Cost effective and clinically effective) • How do we address the epidemiology of smoking. Industrializing tobacco control. Build into ALL care pathways. Critical life points as incentives to quit. Broader tobacco control. • Weight, diet, activity and alcohol consumption are also important risk factors. We don't do enough here • Implementation of preventive interventions should also be equitable. It does not seem to be now (eg smoking cessation) • Big potential for large population gain here – though long term. • CLAN (and lots of others) should champion this among clinicians of all flavours • Age and deprivation structures of populations are very important considerations. Airedale is affluent and old. City is deprived and young To contents
Summary (2) – need. Incidence, survival and mortality. Need – incidence survival and mortality. • incidence and mortality rates (Lung) increased dramatically with age • There are important differences in cancer incidence, mortality (and survival in some cancers, but NOT lung) across socioeconomic groups. Work to reduce health inequalities in cancer needs to take these trends into account. • Much of the observed difference in mortality between deprivation categories (all cancers) is explained by lung cancer (inequalities in smoking?) • Mortality rates for lung cancer in men fell significantly over the decade from 1991 - 2000 for all deprivation categories. • In contrast, lung cancer mortality in women showed a small increase overall (significant differences in mortality by socio-economic group remained). • Change in the pattern of smoking prevalence over time? Men quitting more? • There is limited evidence of a survival gap between most / least deprived. If there is a socio economic gap, it is not statistically significant. No ethnicity data. To contents
Summary (3) – Screening and early diagnosis. Staging • Little is known about stage at presentation for Lung (or others) • A range of further analysis will be undertaken with the LUCADA audit dataset, possible links into other data sources. This is highlighted in the notes page below. • Likely to show socio economic difference in staging at presentation (or Dx) • This leads to consideration of the implementation of a range of early Dx strategies – • Sx education – clinician and public. Culturally aware. Literacy. market and message segmentation; use of peers etc etc • earlier referral – might be warranted…….is there evidence that this will make the difference to survival or mortality rates………….not sure…..but certainly a need to key into the pilots mentioned in Ca Reform Strategy – are we one of them • Clinical culture - referral to exclude a diagnosis • Community diagnostics? Do we need to be smarter about how we route people to diagnostics quickly? • How well do we make use of whatever screening monitoring data we can get to monitor equality of uptake. • In cervical cancer, there is a large observed variation in screening coverage at practice level. Some population characteristics and some health care system characteristics are factors in this. This is an area NSC are currently activiely exploring. This needs to be carefully considered by CLAN To contents
Summary (4) – service provision and system performance. Service Provision, treatment use and performance • analysis of service provision is difficult to interpret in terms of equity, as elements of service provision are affected by many factors Treatments • There is some evidence of variation in service provision related to geography and age, but not socio economic status. This does not take into account stage at presentation, co morbidities or other clinically relevant factors (each of which could confound). Thus it is difficult to draw firm conclusions about treatment variation (and whether this has an impact on outcomes) without further analysis • These variations did not appear to relate to, or translate to need as measured by mortality or incidence. • The variations found may actually relate primarily to provider variation across West Yorkshire. • This analysis uses YHPHO Equity Audit from 2002. It is likely that variations in system performance (and possibly treatment used) have equalised over time – National Standards. • Wide range of factors relating to the performance of a cancer system not fully considered. prevention as well as other measures of treatment and service provision– e.g. primary care provision, staffing numbers, survival rates • The system performance measures will undoubtedly have changes (62 days / 2 weeks etc etc) – may be scope for updating some of this analysis. • Whether a huge focus in this area will acheive significant improvements in health outcomes (population wide or addressing the equality gap) should be seriously considered. The largest gain will come from industrial scale prevention and early diagnosis strategies. To contents
Populations To contents
We have a younger population than E&W To contents
Age profile of the population • Age is a significant factor in Cancer • Age Profile not equally spread through the district To contents
We have a more ethnically diverse population than E&W. Update? Do we have more up to date info on Black pop – WYCSA getting some on new reg with GP by district and country of origin…GF sourcing this To contents
Not strictly a risk factor, but a common measure of equality of outcomes 43% of Bradford's population live in the most deprived 20% of areas in England. Meaning Bradford has more than double the expected proportion of people living in the most deprived areas compared to E&W. The age structure in the most deprived quintiles is significantly different This has a bearing on cancer - making interpretation of data more complex. Bradford also has some of the most affluent areas across the country Deprivation in Bradford by IMD 2004 Quintiles To contents
10,100 new patients registering from overseas in Bradford. NB treat data with suspicion until we know more!!!! We know very little about this population. New Entrants To contents
Common risk factors to all Cancers. To contents
Close correlation with deprivation There is limited tobacco control data: either implementation of tobacco control or smoking cessation data below the level of the whole population (SHA return on smoking cessation) Smoking - % Prevalence To contents
Smoking – Adults. A more detailed consideration To contents
There is other data on smoking prevalence and quitting available through the QOF. Interpret it with care • Correlation between deprivation and smoking prevalence. • NB ONLY pt on a dis register. We don’t know about those that are not on a register. • No clear correlation between % offered referral and deprivation. All referring well. To contents
Obesity - % prevalence. To contents
Binge Drinking - % prevalence To contents
Fruit and Veg - % of adult population consuming >5 portions per day. To contents
Screening • Beverly – what Sc data do we have??? • To ADD! To contents
All Cancers To contents
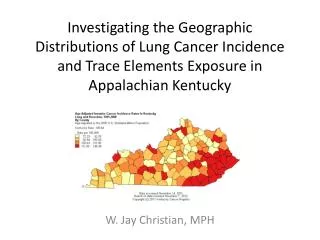
Remember we have a younger, but more deprived population overall. This analysis is adjusted for age structure. District level analysis might mask sub population effect. Bradford is second most deprived district in YH. Spearhead areas have stat signif higher prevalence DSR Mortality from All Cancers – All Cancers. PCT level To contents
How does Bradford compare. Incidence • Adjusted for age structure – ie DSR • PCT level analysis might mask sub population effect. To contents To contents
How does Bradford compare. Mortality • Adjusted for age structure – ie DSR • PCT level analysis might mask sub population effect. To contents
Adjusted for age In both sexes – higher prevalence in YH than in England. Bradford will be no different, and most likely higher than YH (deprivation profile). DSR Mortality from all cancers is decreasing over time. YH rate is higher than national. Bradford district, likely higher than YH To contents
Cancer mortality. All sites. Old PCT. Trends over 9 years • A relatively static trend in Cancer mortality (all sites) when analyzed by old PCT. • NB these are crude rates, using 2003 registered population for all years (for simplicity). • Not standardized for age structure (a significant confounder). • Airedale has the oldest population – but is least deprived. City has the youngest population but is most deprived. • Confidence intervals are not plotted here. It is likely there would be no statistically significant differences. To contents
Ca Prevalence at practice level. Raw prevalence. QOF 07 08 • This is the raw QOF Prevalence. • No account of age structure in practice populations • Many weaknesses in interpretation of this data. Many data quality issues. To contents
Age standardising will probably not help. Data quality is too weak to support drawing any conclusions from a standardisation model. Airedale is oldest, least deprived. City youngest most deprived. To contents
Lung Cancer Risk Factors Incidence Stage at Dx Treatment Survival Mortality To contents
Risk Factors To contents
Estimated prevalence of smoking. To contents
NB – correlation with deprivation in Bradford by IMD 2004 Quintiles To contents
Incidence To contents
Falling Nationally. Relatively static in WY. Reflects historic trends in smoking prevalence and smoking cessation Incidence – national and WY To contents
Unadjusted for age profile No deprivation data. Trends in incidence have an approximate correlation with deprivation profile of old PCTs. Incidence at ‘old PCT’ level. To contents
Principally prevalent >50yrs. Much higher >75 yrs Incidence and age To contents
Stage at diagnosis To contents
No data!! YET!. More to be added here. LUCADA. • Well certainly not much high quality data that is ‘routinely available’ • NYCRIS view is that the q of the data in this area (particularly for Lung) is poor. • Either stage at Dx or presence of mets at Dx • Clini audit might get us a better answer, but labour intensive. • Clinicians gut feel for this issue – qualitative evidence. Worth adding in if there is a means to assess systematically. • LUCADA information might help elaborate this further. To contents
Treatment for Lung Ca To contents
There is (was – this is old data) variation in waiting time to Dx for GP referred patients. 2002. A greater proportion referred quickly in N and S&W compared to Airedale and City. Has this changed? Waiting Times – GP referral to diagnosis‘old PCTs’. Lung To contents
Variation in waiting time to diagnosis for patients referred by their GP by deprivation quintile in 2002. The most affluent quintile (46%) were most likely to wait less than 2 weeks from referral to diagnosis, Little evidence of socio – economic gradient across all other groups. 2002 Data. Has this changed. All W Yorks Waiting Times – GP referral to diagnosis. Deprivation Quintiles. Lung To contents
Similar variation in diagnosis to treatment. 2002 data. Has this changed? Waiting Times - diagnosis to treatment- ‘old PCTs’ . Lung To contents
There is inequality in wait from Dx to Rx In diagnosis to treatment times by deprivation quintile, 42% of the most affluent quintile waiting less than four weeks from diagnosis to first treatment compared with 29% in the most deprived quintile. 2002 data. All W Yorkshire. Has this changed. Waiting Times - diagnosis totreatment. Deprivation quintiles. Lung To contents
In 2002, 51% of persons diagnosed with lung cancer received treatment for the disease, with males and females equally likely to have received similar treatment. There is a direct relationship between age and treatment, with 82% of persons aged under 50 and 34% of persons aged over 75 receiving treatment. Most treatment types reduced with age: persons aged under 50 were most likely to receive chemotherapy, and the group aged 50-74 were more likely to receive radiotherapy. Treatment for Lung Cancer To contents
V few (4.9%) Bradford City receive surgery - ?late presentation. But not explained by deprivation alone – compare to S Leeds. 5.9% Airedale patients receive RT Geographic variation in treatment modalities. Lung To contents
The poor less likely to be treated. When aggregated into deprivation quintiles, limited difference in actual treatment type. Certainly – unlikely to be statistically significant. Treatment and Deprivation. Lung To contents