Download
1 / 12
120 likes | 239 Views
Wisconsin: A PCIP Case Study October 7, 2010. HIRSP Authority. The Health Insurance Risk-Sharing Plan (HIRSP) is Wisconsin’s state high-risk pool. HIRSP has been operational since 1980 and has been administered by the HIRSP Authority since July 1, 2006.

E N D
Wisconsin: A PCIP Case Study October 7, 2010
HIRSP Authority • The Health Insurance Risk-Sharing Plan (HIRSP) is Wisconsin’s state high-risk pool. • HIRSP has been operational since 1980 and has been administered by the HIRSP Authority since July 1, 2006. • Current enrollment in HIRSP (not including PCIP) is 18,265.
HIRSP Premiums • Historically, premiums were estimated to be 140%-150% of the standard risk in the private market for a comparable plan. In 2008 and for 2009, HIRSP premiums were approximately 120% of the standard risk in the private market. • In 2010, composite premiums are estimated to be close to 100% of the standard risk for policies in force in the commercial market. • Premiums will not increase in 2011.
HIRSP Federal • HIRSP signed a contract with HHS in early July and applications were available July 15th. • In order to stretch Wisconsin’s allocation to serve maximum number of eligibles (est. 8,500), decision made to pay provider’s Medicaid rates for HIRSP Federal plans. • In order to make HIRSP Federal plans as affordable as possible, “standard risk” premium calculated from “new issue” rates and adjustment to reflect HIRSP’s unique administrative structure. • In order to address diverse needs of eligible population, four deductible options offered: $500, $1,000, $2,500 and $3,500.
HIRSP FederalPremiums • HIRSP Federal premiums are among the lowest in the country. Premiums vary by deductible plan and are illustrated for two most popular plans: HIRSP Federal 2,500 • 24 and Under: $127 • 25-29: $134 • 30-34: $152 • 35-39: $181 • 40-44: $215 • 45-49: $266 • 50-54: $330 • 55-59: $405 • 60+: $474 HIRSP Federal 3,500 • 24 and Under: $106 • 25-29: $113 • 30-34: $128 • 35-39: $152 • 40-44: $181 • 45-49: $223 • 50-54: $277 • 55-59: $340 • 60+: $398
Key Differences Key Differences Between HIRSP and HIRSP Federal • Six month uninsurability for HIRSP Federal • Low-income subsidy program for HIRSP • No pre-existing condition waiting period for HIRSP Federal • Plan Choice: HIRSP Federal offers a $500 deductible option and HIRSP offers a $5,000 deductible option. Choosing Plans: Someone who has been uninsured for six months will most likely do better in HIRSP Federal; however, if the applicant is low-income they should consider both plans.
HIRSP Federal Plans • To date 300 applications have been received, which is less than expected. • While uptake for HIRSP Federal has been slower than expected, HIRSP is growing quickly. • September 2010: 101 HIRSP Federal applications compared to 674 HIRSP applications.
Commonalities • Members in both HIRSP and HIRSP Federal have demonstrated a preference for low-premium, high-deductible products. Members in HIRSP have shown preference for plans with first dollar coverage (e.g. non-HSA plans)
Differences • Members in the federal pool are younger than members in HIRSP. Average age in HIRSP Federal is 48 years compared to 53 years in HIRSP. Members under age 30 represent 16% of HIRSP Federal membership. • Members in the federal pool have lower income than members in HIRSP. In HIRSP federal 50% of members report income under $33,000 and only 5% report income over $75,000. In HIRSP, 25% of members are subsidized and have income under $33,000 and 10% have income over $100,000. • Claims data is not available yet, but contrary to expectations, application data suggests that morbidity of federal members will be as high or higher than HIRSP members. HIRSP Federal members have a 13% prevalence of cancer and 15% prevalence of mental health/AODA diagnoses. Almost 60% of HIRSP Federal members submitted applications identifying more than one diagnosis. One member is on a waiting list for a heart transplant. • leukopenia, hypertension, alcohol, allergies, depression, spinal stenosis, colon polyps • iliac aneurysm, elevated liver enyzmes, high blood pressure/cholesterol,lung nodules • kidney cancer, anxiety, GERD, blood pressure
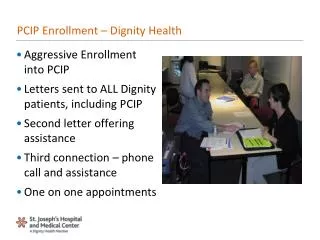
Marketing and Outreach • While work is underway to develop a comprehensive marketing campaign, a variety of marketing and outreach initiatives targeted to consumers, agents, advocates and health care providers have been undertaken: • Two mailing to low-income (under 200% FPL) childless adults on state program waiting list (1st 45,000; 2nd 65,000). • Multiple communications to licensed insurance agents. • Rejection letters include notification about HIRSP. • Notification to network health care providers. • Training of Milwaukee area health care providers and consumer advocates. • Three trainings of benefit specialists across the state. • Multiple communications to state legislators. • Information packets to disease and consumer organizations and FQHCs. • Public Affairs cable program interview. • Multiple newspaper stories.
What Can be Learned? • To attract members - the PCIP plans should offer a range of plan designs including, at a minimum, at least one non-HSA plan. • Low-income Americans are more likely to be uninsured and may be more likely to seek out coverage in the PCIP when needed. Keeping the PCIP premiums affordable and possibly obtaining a law change to allow low-income subsidy could be beneficial. • Individuals who have been uninsured for at least six months may have created mechanisms for managing their health (e.g. using community clinics and generic drug programs). It may take considerable education in addition to traditional outreach strategies to entice these individuals to purchase coverage. • More data is needed to understand whether low-enrollment is a function of lack of knowledge or whether it is a function of the plan design (e.g. six month “go bare” requirement or premium affordability).
Contact Information Amie Goldman CEO, HIRSP Authority Chair, NASCHIP agoldman@hirsp.org (608) 441-5777 www.hirsp.org