Download
1 / 14
150 likes | 278 Views
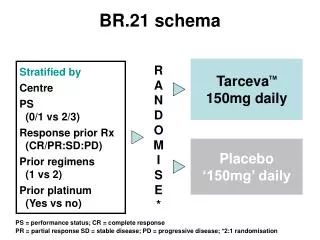
BR.21 Study Design. Stratified by: Centre PS, 0/1 vs 2/3 Response to prior Rx (CR/PR:SD:PD) Prior regimens, (1 vs 2) Prior platinum, (Yes vs no). Erlotinib * 150mg/day. R. * 2:1 Randomization. Placebo “150 mg” daily.

E N D
BR.21 Study Design Stratified by: Centre PS, 0/1 vs 2/3 Response to prior Rx (CR/PR:SD:PD) Prior regimens, (1 vs 2) Prior platinum, (Yes vs no) Erlotinib* 150mg/day R *2:1 Randomization Placebo “150 mg” daily Shepherd et al. N Engl J Med. 2005;353:123-132.
BR.21 Progression-Free Survival ___ Erlotinib, _____ Placebo 2.2 mos 1.8 mos *HR 0.61, p <0.0001 *Adjusted for stratification factors (except centre) AND EGFR status Months Shepherd et al. N Engl J Med. 2005;353:123-132.
BR.21: Overall Survival 1.00 0.75 0.50 0.25 0 HR=0.70 (95% CI, 0.58-0.85); P < 0.001* *HR and P-value adjusted for stratification factors at randomization plus HER1/EGFR status. Survival distribution function 31% 42.5% improvement in median survival Erlotinib Placebo 21% 0 5 10 15 20 25 30 Survival time (months) Shepherd et al. N Engl J Med. 2005;353:123-132.
IPASS Study Design Gefitinib 250mg/day • Chemonaïve advanced NSCLC • Adenocarcinoma • Non-smoker or light smoker • N = 1217 R Paclitaxel (200 mg/m2, IV, d1) plus carboplatin (AUC=5 or 6 mg/min) repeated every 3 weeks up to 6 cycles Primary endpoint: PFS Secondary endpoints: ORR, OS, QoL and safety Mok TS, et al. N Engl J Med. 2009 Sep 3;361(10):947-57.
IPASS: PFS and OS by Known EGFR Mutation Status Gefitinib EGFR M+ Gefitinib EGFR M- C / P EGFR M+ C / P EGFR M- 4 8 12 16 20 24 PFS (2008) OS (2010) 1.0 1.0 0.8 0.8 Mutation + 0.6 0.6 Probability of survival 0.4 0.4 Probability of progression-free survival 0.2 0.2 Mutation - 0.0 0.0 0 4 8 12 16 20 24 28 32 36 44 48 0 40 Time from randomisation (months) Time from randomisation (months) 52 Patients at risk excludes censored patients and those who have experienced an event Yang CH et al. ESMO 2010
INTEREST Study Design Endpoints • Patients • Age ≥18 years • Life expectancy≥8 weeks • Progressive or recurrent disease following CT • Considered candidates for further CT with docetaxel • 1 or 2 CT regimens(≥1 platinum) • PS 0-2 • Primary • Overall survival(co-primary analysesa of non-inferiority in all patients and superiority in patients with high EGFR gene copy number) • Secondary • Progression-free survival • Objective response rate • Quality of life • Disease-related symptoms • Safety and tolerability • Exploratory • Biomarkers IRESSA 250 mg/day 1:1 randomization Docetaxel 74 mg.m2 every 3 weeks aModified Hochberg procedure applied to control for multiple testingCT: chemotherapy; PS: performance status Kim ES, et al. Lancet. 2008 Nov 22;372(9652):1809-18.
INTEREST: Gefitinib vs. Docetaxel in NSCLC After Chemotherapy Gefitinib demonstrated non-inferior survival compared with docetaxel OS in overall study population OS in patients with high EGFR gene copy number 1.0 0.8 HR (96% CI) = 1.020 (0.905, 1.150) HR (95% CI) = 1.09 (0.78, 1.51) P = 0.6199 0.6 Probability of survival Gefitinib Docetaxel 0.4 0.2 0.0 20 36 40 20 40 0 0 Months Months Kim ES, et al. Lancet. 2008 Nov 22;372(9652):1809-18.
SATURN Study Design • Run-in Period: • Patients with advanced NSCLC • Treatment with four cycles of platinum-doublet chemo • N = 1949 Erlotinib 150mg/day • Eligibility: • No progressive disease • N = 889 R Placebo Primary endpoint: PFS in all patients; PFS in patients with EGFR IHC-positive tumours Secondary endpoints: OS in ITT and EGFR-positive tumours, PFS in EGFR-negative tumours, time to progression, tumour response, QoL Cappuzzo F, et al. Lancet Oncol. 2010 Jun;11(6):521-9.
SATURN: Erlotinib vs. Placebo in NSCLC After Chemotherapy OS PFS 1.0 0.8 0.6 0.4 0.2 0 1.0 0.8 0.6 0.4 0.2 0 Erlotinib (n=437) Placebo (n=447) Erlotinib (n=438) Placebo (n=451) HR=0.71 (0.62–0.82) Log-rank p<0.0001 HR=0.81 (0.70–0.95) Log-rank p=0.0088 Probability 0 8 16 24 32 40 48 56 64 72 80 88 96 0 8 16 24 32 40 48 56 64 72 80 88 96 Time (weeks) Time (weeks) Cappuzzo F, et al. Lancet Oncol. 2010 Jun;11(6):521-9.
SATURN: EGFR Activating Mutations PFS1 OS2 1.0 0.8 0.6 0.4 0.2 0 1.0 0.8 0.6 0.4 0.2 0 HR=0.10 (0.04–0.25)Log-rank p<0.0001 HR=0.83 (0.34–2.02)Log-rank p=0.6810 Probability 0 3 6 9 12 15 18 21 24 27 30 33 36 0 8 16 24 32 40 48 56 64 72 80 88 96 Time (months) Time (weeks) 1. Cappuzzo F, et al. Lancet Oncol. 2010 Jun;11(6):521-9. 2. Brugger, et al. J Thorac Oncol 2009;4 (Suppl. 1):S348–9 (Abs. B9.1)
PFS: Overall Population Dacomitinib versus Erlotinib Phasell Overall population 100 90 80 70 60 50 40 30 20 10 0 PF299804 (n=94) Median: 12.4 weeks (95% CI: 8.3–16.1) Erlotinib (n=94) Median: 8.3 weeks (95% CI: 8.0–11.4) Progression-freesurvival probability (%) Unstratified analysis:Hazard ratio = 0.681(95% CI: 0.490–0.945)Log-rank P-value = 0.019 0 5 10 15 20 25 30 35 40 45 50 55 60 Time (weeks) CI = confidence interval Post-baseline tumor assessments were initiated at week 8 and conducted every 4 weeks thereafter. Boyer et al ASCO 2010. Abstract LBA7523.
AFATINIB: PRECLINICAL ACTIVITY 1. Oncogene 2008;27:4702-4711. 2.Cancer Res 2006;66:8163-71. 3. Science 2004;304:1497. 4. JNCI 2005;97:1185-94. 5. Cancer Res 2007; 67:11924-32.
PFS by independent review Statistically significant across almost all subgroups