Download
1 / 1
20 likes | 88 Views
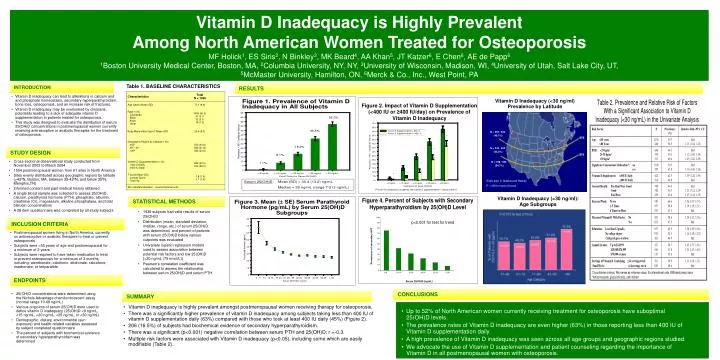
This study examines the prevalence of vitamin D inadequacy in postmenopausal women undergoing osteoporosis treatment. Results show high rates of inadequacy and risk factors associated with low vitamin D levels. The study emphasizes the importance of supplementation and patient education.

E N D
N = 259 / 532 (48.7%) N = 342 / 642 (53.3%) N = 198 / 362 (54.7%) Vitamin D Inadequacy is Highly Prevalent Among North American Women Treated for OsteoporosisMF Holick1, ES Siris2, N Binkley3, MK Beard4, AA Khan5, JT Katzer6, E Chen6, AE de Papp61Boston University Medical Center, Boston, MA, 2Columbia University, NY, NY, 3University of Wisconsin, Madison, WI, 4University of Utah, Salt Lake City, UT, 5McMaster University, Hamilton, ON, 6Merck & Co., Inc., West Point, PA Table 1. BASELINE CHARACTERISTICS INTRODUCTION RESULTS • Vitamin D inadequacy can lead to alterations in calcium and and phosphate homeostasis, secondary hyperparathyroidism, bone loss, osteoporosis, and an increase risk of fractures. • Vitamin D inadequacy may be overlooked by clinicians, potentially leading to a lack of adequate vitamin D supplementation in patients treated for osteoporosis. • This study was designed to evaluate the distribution of serum 25(OH)D concentrations in postmenopausal women currently receiving antiresorptive or anabolic therapies for the treatment of osteoporosis. Vitamin D Inadequacy (<30 ng/ml) Prevalence by Latitude STUDY DESIGN • Cross-sectional observational study conducted from November 2003 to March 2004 • 1554 postmenopausal women from 61 sites in North America • Sites evenly distributed across geographic regions by latitude (>42ºN, Boston, MA, between 35-42ºN, and below 35ºN, Memphis,TN) • Informed consent and past medical history obtained • A single blood sample was collected to assess 25(OH)D, calcium, parathyroid hormone (PTH), phosphate, albumin, creatinine (Cr), magnesium, alkaline phosphatase, and total bilirubin concentrations • A 28 item questionnaire was completed by all study subjects Sites also in Alaska and Hawaii P = NS for test of trend STATISTICAL METHODS Vitamin D Inadequacy (<30 ng/ml): Age Subgroups • 1536 subjects had valid results of serum 25(OH)D • Distribution (mean, standard deviation, median, range, etc.) of serum 25(OH)D was determined, and percent of patients with serum 25(OH)D below various cutpoints was evaluated • Univariate logistic regression models used to assess association between potential risk factors and low 25(OH)D [<30 ng/mL (75 nmol/L)] • Pearson’s correlation coefficient was calculated to assess the relationship between serum 25(OH)D and serum PTH INCLUSION CRITERIA • Postmenopausal women living in North America, currently on antiresorptive or anabolic therapies to treat or prevent osteoporosis • Subjects were >55 years of age and postmenopausal for a minimum of 2 years • Subjects were required to have taken medication to treat or prevent osteoporosis for a minimum of 3 months, including: alendronate, calcitonin, etidronate, raloxifene, risedronate, or teriparatide ENDPOINTS CONCLUSIONS • 25(OH)D concentrations were determined using the Nichols Advantage chemiluminescent assay (normal range 10-68 ng/mL) • Various cutpoints of serum 25(OH)D were used to define vitamin D inadequacy (25(OH)D <9 ng/mL, <15 ng/mL, <20 ng/mL, <25 ng/mL, or <30 ng/mL) • Demographic, dietary, environmental (sun exposure) and health-related variables assessed by subject completed questionnaire • The percent of subjects with biochemical evidence of secondary hyperparathyroidism was determined SUMMARY • Vitamin D inadequacy is highly prevalent amongst postmenopausal women receiving therapy for osteoporosis. • There was a significantly higher prevalence of vitamin D inadequacy among subjects taking less than 400 IU of vitamin D supplementation daily (63%) compared with those who took at least 400 IU daily (45%) (Figure 2). • 206 (16.5%) of subjects had biochemical evidence of secondary hyperparathyroidism. • There was a significant (p<0.001) negative correlation between serum PTH and 25(OH)D; r =-0.3. • Multiple risk factors were associated with Vitamin D inadequacy (p<0.05), including some which are easily modifiable (Table 2). • Up to 52% of North American women currently receiving treatment for osteoporosis have suboptimal 25(OH)D levels. • The prevalence rates of Vitamin D inadequacy are even higher (63%) in those reporting less than 400 IU of Vitamin D supplementation daily. • A high prevalence of Vitamin D inadequacy was seen across all age groups and geographic regions studied. • We advocate the use of Vitamin D supplementation and patient counseling regarding the importance of Vitamin D in all postmenopausal women with osteoporosis.