Download
1 / 81
1.42k likes | 2.83k Views
Mass Casualty & Disaster Triage. Amy Gutman MD prehospitalmd@gmail.com. Overview. Disasters & MCIs Triage Pediatrics WMD Incident Command Lessons Learned. Disasters Are Different. Defining a Disaster. What Is A Disaster?.

E N D
Mass Casualty & Disaster Triage Amy Gutman MD prehospitalmd@gmail.com
Overview • Disasters & MCIs • Triage • Pediatrics • WMD • Incident Command • Lessons Learned
Disasters Are Different Defining a Disaster
What Is A Disaster? • Any event, regardless of size or expanse, that overwhelms available resources • Any disaster can trigger a health crisis • Initial disasters are often compounded by poor planning & communications, costing time, resources, & lives • Daily emergency care is not usually constrained by resource availability • In daily emergencies, you do the best for the individual • In disasters, you do the greatest good for the greatest number
Murrah Federal Building Oklahoma City, OK 168 dead, >800 injured Van vs Train New Zealand 2 dead, 6 critical, 2 stable patients
“A single death is a tragedy; a million deaths is a statistic.” Josef Stalin • Air Force Base • Airports • Bridges • Chemical Plants • Hospitals • Ohio River • Skyscrapers • Sports Arenas • Train Depot • Universities • Weather
Disaster “MCI” Categories • I “Expanded Medical Incident” • >10 critical, <50 patients • Local resources available to treat injured • II “Major Medical Incident” • >50 critical, <200 patients • Regional resources available to treat injured • III “Disaster” • >200 patients of any type • Lack of regional resources available to treat injured • State, Federal resources required
MCI LEVEL I County Fire District Chief 5 ALS units 5 Fire companies 2 ALS helicopters 1 Logistics officer & supply trailer Communications Chef 1 PIO MCI LEVEL II County fire District Chief 10 ALS, 3 BLS units 7 Fire companies 3 ALS helicopters 2 Transit buses 2 Logistics Officers, 2 supply trailers 2 Communications Chiefs 1 PIO MCI LEVEL III County FD Rescue Supervisors 15 ALS, 5 BLS units 10 Fire Companies All available ALS helicopters 4 transit buses 3 Logistics Officers, 3 supply trailers 2 Communications Chiefs 1 PIO MCI LEVEL IV County FD Rescue Supervisors 20 ALS, 10 BLS units 15 Fire companies All available helicopters 6 transit buses 4 Logistics officers, 4 supply trailers 2 Communications Chiefs 1 PIO MCI Response: Brevard County
Code Black Bomb Threat Code Gray Severe Weather Code Orange Haz Materials Incident Code Yellow Disaster Disaster Emergency Codes
What is Triage? • “Triage” means “to sort” • A process in which victims are sorted into groups; priorities of care established & resources allocated • Looks at medical needs & urgency of each individual • Sorting based on limited data acquisition & resource availability to get care to those who need it and will benefit from it the most • Provides an objective framework for stressful & emotional decisions
Triage Organizes Priorities • “Normal” Circumstances • Use all available manpower & supplies to save a few lives • Minor injuries receive immediate care • Severe injuries receive immediate care • Mortal injuries may or may not receive care • “Disaster” Circumstances • Number of injured > ability to treat in normal manner • Resource use focuses on saving as many lives as possible • Minor injuries wait for care • Severe injuries receive immediate care • Mortal injuries do not receive care
Disaster Ethical Considerations • Alteration of standards of care • “Utilitarian rule" governs medical care • The greater good of the greater number rather than the particular good of the individual • A. Jonsen and K. Edwards, “Resource Allocation” in Ethics in Medicine, Univ. of Washington School of Medicine
Triage is Dynamic • Primary Triage is performed close to incident in a “safe” area • Secondary Triage is performed in a separate area by a second set of medical personnel • Tertiary Triage is performed either in the Secondary Triage area, or at the destination facility
Primary Triage • Sort patients based on need for immediate care • Assumptions: • Medical needs outstrip immediately available resources • Additional resources will become available with time • Triage based on physiology • How well the patient is able to utilize their own resources to deal with their injuries • Which conditions will benefit the most from the expenditure of limited resources
Secondary Triage • Match patients’ current & anticipated needs with available resources • Incorporates: • A reassessment of physiology • Initial treatment & assessment of patient response • Further knowledge of resource availability • Goal is to distinguish between: • Victims needing life-saving treatment in a hospital setting • Victims needing life-saving treatment initially available on scene • Victims with non-life-threatening injuries, at risk for delayed complications • Victims with minor injuries
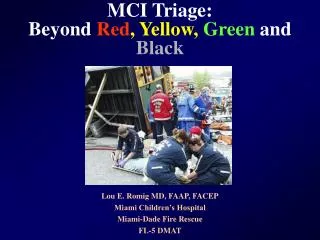
NATO Secondary Triage Injury Categories • Green • Minor lacerations, contusions, sprains, superficial burns • Yellow • Open abdominal wound, eye injury, pulseless limb, fractures, significant burns other than face, neck or perineum • Red • Airway obstruction, cardio-respiratory failure, external hemorrhage, shock, open chest wound, burns of face or neck • Black • GCS<8, burns >85% BSA, multisystem trauma, signs of impending death
Tertiary Triage • Goal is to optimize individual outcome • Incorporates: • Sophisticated assessment & treatment • Further assessment of available medical resources • Determination of best venue for definitive care
Basic Disaster Life Support • National Disaster Life Support Education Consortium, via Medical College of Georgia’s Center of Operational Medicine • Disaster Medicine Online University (www.dmou.org) • Endorsed by the AMA & NREMT • MASS Triage • Move • Assess • Sort • Send • ? Assessment guidelines or Pediatric considerations
START: Simple Triage & Rapid Treatment • Prepares emergency personnel to quickly organize their resources to handle multi-casualty emergencies by assuming predetermined roles • Based upon ambulatory status, respirations, pulse, & mentation • Does not require any medical equipment • Provides a rapid assessment of resource needs • Developed jointly by Newport Beach (CA) Fire & Marine Department & Hoag Hospital • Gold standard for field adult multiple casualty (MCI) triage in the US and numerous countries around the world
START Problems • Does not take resources into account • Some are more “Red” than others • Uses a limited number of physical parameters (RPM) • Not commonly used during daily operations
Triage Categories • Green • Minor injuries that can wait for longer periods of time for treatment • Yellow • Potentially serious injuries, but are stable enough to wait a short while for medical treatment • Red • Life-threatening but treatable injuries requiring rapid medical attention • Black • Dead or still with life signs but injuries are incompatible with survival in austere conditions
Triage Flow Chart • Separate walking wounded from others • Use physiology to assess: • Breathing • Blood flow • Mental status
All Walking Wounded Are “Green” • If not walking & talking, begin assessing life functions
Breathing • Cannot breathe on own after airway opened = BLACK • Breathing rapidly = RED • Breathing regularly = go to next step in flow chart
Perfusion • If radial pulse = go to “Mental Status” • If no radial pulse, check capillary refill • If refill >2 secs = RED • If refill <3 secs = go to “Mental Status”
Mental Status • Cannot follow simple command = RED • Can follow simple command = YELLOW • All victims have now completed primary triage
Walking Wounded = Green • All green pediatric patients must be immediately re-assessed in secondary triage • May have been carried to the secondary triage area & have not proven their physiologic stability
Breathing • Position the upper airway of the apneic child • If breathing = RED
Perfusion • If the child doesn’t start breathing with upper airway opening, feel for a pulse • If no pulse is palpable = BLACK
Perfusion • If the patient has a pulse, give 5 breaths to open the lower airways • If no ventilations = BLACK • If breathing = RED
Ventilation • If respiratory rate is <15 or >45 = RED • If respirations are > 15 or <45, move on to next step
Perfusion • If no palpable pulse = RED • If pulse is present, move to the next step
Mental Status • If patient is inappropriately responsive to pain, posturing, or unresponsive = RED • If patient is alert, responds to voice or appropriately responds to pain = YELLOW
Nonambulatory Children • Patient can still be GREEN if no external signs of trauma, breathing spontaneously, positive pulse & normal vitals • If patient has minor external trauma not involving the head, but otherwise stable vitals, then tag as YELLOW • If patient meets any red criteria, then tag as RED • If patient has no pulse, no spontaneous respirations after 5 breaths, or significant external trauma, then tag as BLACK
WMD Triage Challenges • Any triage model for WMD must consider decontamination • Patients with injuries from a conventional attack in addition to a chemical, radiological, or nuclear exposure • Difficulty of conducting patient assessment & care with responders in protective gear • Biological agents impact field triage & potentially the destination facility • Patterns of EMS calls may assist in identification of a occult biological agent attack or a natural epidemic • Example biosurveillance tool is the First Watch program http://www.stoutsolutions.com/firstwatch
WMD Triage Challenges • Some agents cause “toxindromes” that allow for prediction of outcome based on presenting symptoms and signs • Agent-specific triage is dependent upon strong suspicion of the agent’s use • Very difficult to train & maintain readiness with multiple agent-specific triage schemes
Nerve Agents Triage • Red: • Seizures, multisystem symptoms: GI, neuromuscular, respiratory – excluding eyes & nose • Black: • Pulseless or apneic, respiratory failure
Phosgene & Vesicants Triage • Red: • Moderate to severe respiratory distress, only when intensive resources are immediately available • Black: • Burns >50% BSA from liquid exposure, signs of more than minimal pulmonary involvement, when intensive resources are not available
Cyanide Triage • Red: • Active seizure or apnea with preserved circulation • Black: • No palpable pulse
Key Points about MCI Triage • Anything that can organize the response to an MCI is useful, including drills • MCI triage is different than daily triage, in both field & ED settings • Resource availability is the limiting factor in MCI triage • In order for MCI triage to work toward its goal, all victims must have equal importance at the time of primary triage • No patient group can receive special consideration other than that dictated by their physiology • MCI triage will never be logistically, intellectually, or emotionally easy, but we must be prepared to do it using the best of our knowledge and abilities
Triage & Treatment Protocols • Must develop protocols BEFORE they are needed • Keep protocols and treatment plans up-to-date • Practice triage method • Practice getting organized to do triage • Remember: Triage is a continuous process
Resource Allocation Triage Transportation Scene Management Resource Coordination
Scene Assessment & Triage Priorities • Greatest good for the greatest number • Maintain universal blood & body fluid precautions • The initial response team assesses scene for potential hazards, safety & number of victims to determine the appropriate level of response • Notify central dispatch to declare an MCI & need for interagency support as defined by incident level • Identify and designate the following positions as qualified personnel become available: • Incident Command Officer • Communications Officer • Extrication / Hazards Officer • Primary & Secondary Triage Officer • Treatment Officer • Loading/Transportation Officer