Download
1 / 17
170 likes | 352 Views
Cyclosporine A reduces infarct size and has no detrimental effect of LV remodeling in STEMI patients Michel Ovize Cardiology Hospital and Inserm U886 Lyon University, France. Direct stenting. Previous work by Piot et al. (NEJM 2008)

E N D
Cyclosporine A reduces infarct size and has no detrimental effect of LV remodeling in STEMI patients Michel Ovize Cardiology Hospital and Inserm U886 Lyon University, France
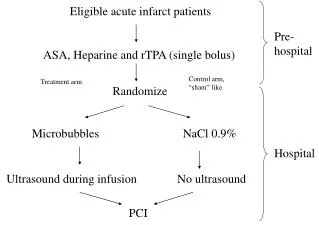
Direct stenting Previous work by Piot et al. (NEJM 2008) Objective: determine whether cyclosporine A can reduce infarct size in STEMI patients STEMI < 12 hrs PCI treatment LAD TIMI flow grade 0-1 No visible collaterals Cyclosporine A (or saline) (2.5 mg/kg, IV bolus) t-10 min t0 Day 1-3 CK / TnI release Infarct size Day 5 MRI Coronary artery occlusion Reperfusion
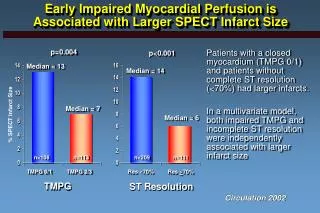
1.4.105 1.2.105 6000 CK release TnI release 1.0.105 5000 0.8.105 AUC (arbitrary units) 250 control 0.6.105 4000 (UI/L) CsA 0.4.105 3000 0.2.105 200 0 2000 10 30 50 70 ACS (%) 1000 150 0 Control Control 24h 60h 4h 12h 30h 8h 16h 20h 36h 42h 48h 54h 66h 72h Adm. CsA CsA 1.2.105 100 CK release TnI release 1.0.105 0.8.105 50 AUC (arbitrary units) 0.6.105 0.4.105 0 66h 72h 12h 4h 8h 24h 30h 60h 20h 54h 16h 36h 42h 48h Adm. 0.2.105 0 0 20 40 60 Reduction of cardiac enzymes release by cyclosporine A Piot et al. NEJM 2008
120 70 60 50 40 area of hyperenhancement (g) * 30 20 10 0 cyclosporine control MRI infarct size (day 5) Piot et al. NEJM 2008;359:473-81
Rationale • CsA can reduce infarct size in STEMI patients. It is therefore expected that this protective effect may be associated with a reduced adverse LV remodeling • However, experimental evidence indicates that CsA, via anti-hypertrophic mechanisms, may favor an adverse remodeling response of the LV after STEMI • We then assessed LV volumes and wall thickness by MRI at 5 days and 6 months after AMI in a population of patients that had received CsA as an adjunct to PCI revascularization
PCI Follow up CMR at 6 months post-MI Cyclosporine A or saline t-10 min t0 Day 5 MRI 6 Month MRI Coronary artery occlusion Reperfusion Mewton et al. JACC 2010
* Control Cyclosporine
Cyclosporine in acute myocardial infarction Mewton et al. (JACC 2010)
PCI Follow up CMR at 6 months post-MI Cyclosporine A t-10 min t0 Day 5 MRI 6 Month MRI Coronary artery occlusion Reperfusion Mewton et al. J Am Coll Cardiol 2010;55:1200–5
There was a significant correlation between left ventricular end-diastolic volume (LVEDV) and infarct size at 6 months (r2=0.40; p<0.05) in the whole group of patients
There was a significant correlation between left ventricular end-systolic volume (LVESV) and infarct size at 6 months (r2=0.66; p<0.05) in the whole group of patients
There was a significant correlation between left ventricular ejection fraction (LVEF) and infarct size at 6 months (r2=0.72; p<0.05) in both groups of patients
MRI at 6 months after cyclosporine-treated MI * * Mewton et al. (JACC 2010)
Conclusion • Cyclosporine used at the moment of acute myocardial infarction reperfusion reduces infarct size and does not have a detrimental effect of LV remodeling. • These results obtained from a limited population of patients must be confirmed by large-scale trials