Download
1 / 21
512 likes | 3.67k Views
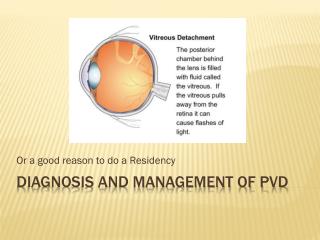
Vitreous & Peripheral Retinal Anomalies. Kelli Shaon, O.D. Posterior Vitreous Detachment. Increases with age Appears as an annular ring floating above the optic nerve (Weiss’ ring) Patient may complain of a new onset of floater(s)

E N D
Vitreous & Peripheral Retinal Anomalies Kelli Shaon, O.D.
Posterior Vitreous Detachment • Increases with age • Appears as an annular ring floating above the optic nerve (Weiss’ ring) • Patient may complain of a new onset of floater(s) • If onset of larger amount of floaters &/or flashes – need to r/o retinal tear or break due to retinal-vitreal traction • A symptomatic PVD, needs to be followed q1 month until symptoms resolve
Vitreous Syneresis • Normal aging process • Is usually more prominent or visible on a patient with a pseudophakia (or IOL) • Is a increased liquefaction of the vitreous • Can see more movement & vitreal strands “fibers” present on examination
Asteroid Hyalosis • A vitreous degeneration in which calcium soaps aggregate in the vitreous • Benign condition – pt usually are completely asymptomatic • More common in older pts • Unilateral ~90% of the time • Often associated with DM or HTN or may be idiopathic • Mgmt: Pt education, Monitor
Lattice Degeneration • Retinal thinning w/ loss of inner retinal tissue • Occurs in 6-10% of general population • More common in myopes • Does have some association of retinal tears, holes, & detachments • Have appearance of criss-crossing “lattice” or sclerosed vessels may or may not be surrounded by pigment
Senile Pigmentary Degeneration • Granular pigment “mottling” seen between the equator & periphery • Benign condition found in up to 20% of those 40+ yo • Often bilateral • Called Senile reticular degeneration – if takes on a reticular or bony spicule appearance
Pavingstone/Cobblestone Degeneration • AKA: 1° Chorioretinal atrophy • Benign condition • More common with aging • Most common in the inferior quadrants • Often bilateral • Often can visualize choroidal vessels • Thought to be an occlusion of choriocapillaris w/ loss of retinal & RPE tissue • Does not predispose to retinal breaks or detachment
White W/O Pressure (WWOP) • Very common retinal finding – up to 30% of general population • Higher incidence in African-Americans • ↑ incidence in myopes • Seen as area of translucent white to grayish discoloration • Has been associated w/ development of retinal tears – So need to monitor
Chorioretinal Scarring • Often associated with old inflammation or trauma • Areas of CR atrophy surrounded by RPE hyperplasia – just needs to be noted • Most important fact is to determine if from active inflammation
RPE window defect • White to yellowish, often round, areas of missing retina • No RPE hyperplasia surrounding • Benign finding • Can be in periphery or posterior pole
Congenital Hypertrophy of RPE (CHRPE) • AKA: Bear tracks if groupings • Flat, discrete darkly pigmented spots • Well defined borders • Can have lacunae present • Location – deep retina • RPE & choriocapillaris • Will not disappear on red-free filter • May have absolute scotoma on VF • Can be associated w/ Gardner’s syndrome (often 4+ lesions)
Choroidal Nevus • AKA: Benign Choroidal Melanoma • Can be anywhere in the retina • Flat but may have overlying drusen (shows presence for some time) • Usually less than 2mmin size • If greater than 2mm then be suspicious of malignancy • Paler grayish color • Non-distinct edges, feathery borders • Disappears with red-free filter (due to location in choroid)
Retinoschisis • Splitting of the sensory retina • OPL from INL • Can be flat or bullous (elevated) • Increased frequency in the elderly • Causes ________ scotoma on VF • Most commonly in inferotemporal quadrant
Retinoschisis • Rarely cause vision loss • Can develop inner & outer layer breaks/holes • Usually inner-layer breaks – larger & clear • Outer layer breaks – smaller & pinker • If both of holes types are present, higher incidence of development of rheg. detachment • Monitor yearly or PRN if holes NOT present in both layers • If holes present in both layers – refer to Retina specialist for laser
Atrophic Retinal hole • A retinal break w/o vitreoretinal traction • Often seen as round red lesion • May have retinal edema &/or RPE hyperplasia surrounding • Management/Follow-up: • Isolate asymptomatic hole – educ. on s/s of RD & f/u 1 yr or PRN • Isolate asymptomatic hole w/ small cuff edema – educ. on s/s of RD & f/u 6 mon or PRN • Isolate asymptomatic hole w/ large cuff edema - retina consult • Symptomatic hole - retina consult
Operculated Retinal Hole • Round red hole w/ overlying floating retinal plug • Vitreal traction is now relieved • Management/Follow-up: • New onset operculum – ed/ on s/s of RD & f/u 6 weeks • Asymptomatic single hole – ed. on s/s of RD & f/u 6-12 months • Asymptomatic multiple hole – ed. On s/s of RD & f/u every 6 months • Asymptomatic w/ large edema cuff (& no RPE hyperplasia) – Retina consult • Symptomatic – (if aphakic or fellow eye has RD or continued traction) – Retina consult
Flap Tear/Horseshoe Tear • Retinal break associated w/ vitreoretinal traction • Tear is red in color w/ grayish retinal tissue surrounding • If horse shoe tear, the point often points toward the post. pole (due to gravity forces of the vitreous) • High likelihood of rheg. RD due to vitreous seaping under retinal break • Management: • Obtain retinal consult to consider laser
Retinal Detachments • Rhegmatogenous: • Separation of the retina from RPE by fluid that enters the subretinal space via retinal breaks • Symptoms: • Sudden onset or increase in floaters • Flashes of light • Changes in peripheral in vision _ “Curtain in vision” • Management: • Fresh RD – immediate retinal consultation • Long-standing – Retina consult w/in 1-2 days
Retinal Detachments • Tractional: • Detachment associated with fibrous retinal & vitreous traction • Most often found with proliferative diseases such a PDR (DM) • Management: • Refer to retina for vitrectomy & possible buckle or laser
Retinal Detachments • Exudative: • From fluid accumulation in the subretinal space • Most often associated with leakage of abnormal blood vessels that have interfered with the normal blood-retina barrier • Examples: • Choroidal melanoma • VKH syndrome • Coat’s syndrome • Exudative ARMD