Download
1 / 1
10 likes | 102 Views
ISOLATED BRAINSTEM SYNDROME AS THE SOLE MANIFESTATION OF NEUROMYELITIS OPTICA SPECTRUM DISORDER

E N D
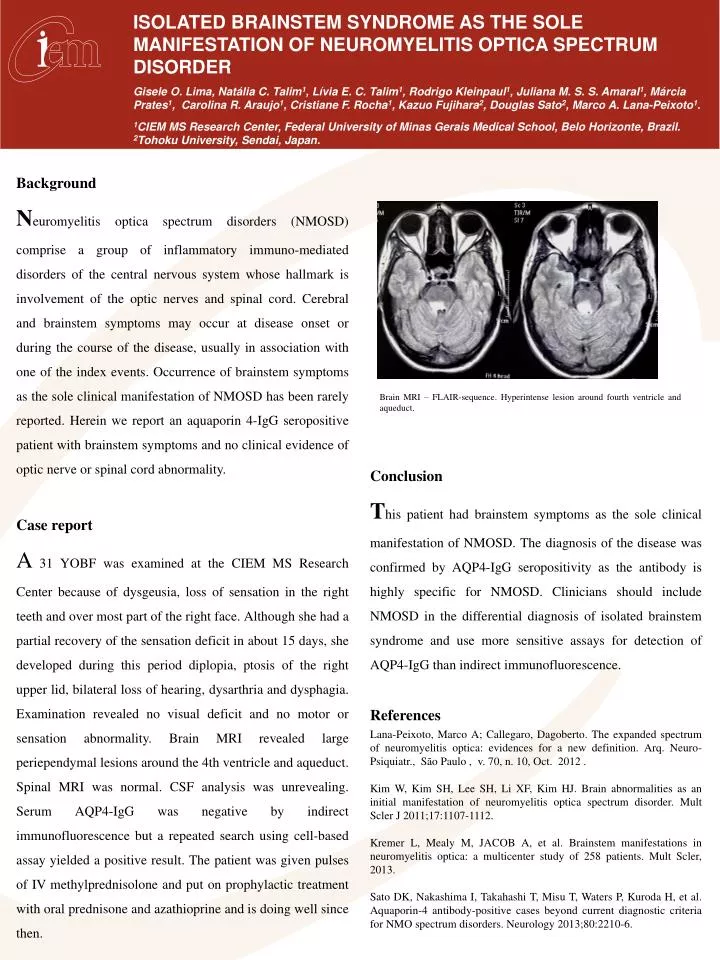
ISOLATED BRAINSTEM SYNDROME AS THE SOLE MANIFESTATION OF NEUROMYELITIS OPTICA SPECTRUM DISORDER Gisele O. Lima, Natália C. Talim1, Lívia E. C. Talim1, Rodrigo Kleinpaul1, Juliana M. S. S. Amaral1, Márcia Prates1, Carolina R. Araujo1, Cristiane F. Rocha1, Kazuo Fujihara2, Douglas Sato2, Marco A. Lana-Peixoto1. 1CIEM MS Research Center, Federal University of Minas Gerais Medical School, Belo Horizonte, Brazil. 2Tohoku University, Sendai, Japan. Background Neuromyelitisoptica spectrum disorders (NMOSD) comprise a group of inflammatory immuno-mediated disorders of the central nervous system whose hallmark is involvement of the optic nerves and spinal cord. Cerebral and brainstem symptoms may occur at disease onset or during the course of the disease, usually in association with one of the index events. Occurrence of brainstem symptoms as the sole clinical manifestation of NMOSD has been rarely reported. Herein we report an aquaporin 4-IgG seropositive patient with brainstem symptoms and no clinical evidence of optic nerve or spinal cord abnormality. Case report A31 YOBF was examined at the CIEM MS Research Center because of dysgeusia, loss of sensation in the right teeth and over most part of the right face. Although she had a partial recovery of the sensation deficit in about 15 days, she developed during this period diplopia, ptosis of the right upper lid, bilateral loss of hearing, dysarthria and dysphagia. Examination revealed no visual deficit and no motor or sensation abnormality. Brain MRI revealed large periependymal lesions around the 4th ventricle and aqueduct. Spinal MRI was normal. CSF analysis was unrevealing. Serum AQP4-IgG was negative by indirect immunofluorescence but a repeated search using cell-based assay yielded a positive result. The patient was given pulses of IV methylprednisolone and put on prophylactic treatment with oral prednisone and azathioprine and is doing well since then. Conclusion This patient had brainstem symptoms as the sole clinical manifestation of NMOSD. The diagnosis of the disease was confirmed by AQP4-IgG seropositivity as the antibody is highly specific for NMOSD. Clinicians should include NMOSD in the differential diagnosis of isolated brainstem syndrome and use more sensitive assays for detection of AQP4-IgG than indirect immunofluorescence. References Lana-Peixoto, Marco A; Callegaro, Dagoberto. Theexpandedspectrumofneuromyelitisoptica: evidences for a newdefinition. Arq. Neuro-Psiquiatr., São Paulo , v. 70, n. 10, Oct. 2012 . Kim W, Kim SH, Lee SH, Li XF, Kim HJ. Brainabnormalities as aninitialmanifestationofneuromyelitisopticaspectrumdisorder. MultScler J 2011;17:1107-1112. Kremer L, Mealy M, JACOB A, et al. Brainstem manifestations in neuromyelitisoptica: a multicenter study of 258 patients. MultScler, 2013. Sato DK, Nakashima I, Takahashi T, Misu T, Waters P, Kuroda H, et al. Aquaporin-4 antibody-positive cases beyondcurrentdiagnosticcriteria for NMO spectrumdisorders. Neurology 2013;80:2210-6. V V Brain MRI – FLAIR-sequence. Hyperintense lesion around fourth ventricle and aqueduct.