Download
1 / 1
10 likes | 190 Views
Heart failure as an initial manifestation of antiphospholipid syndrome . KY. Juarez Escobar 1 , J E. Cruz 1 , J. Vargas Penafiel 1 , M. Jimenez Cruz 1 , J. Gomez Leon 1 , A. Lara Olivares 1 , R . Baleon Espinoza 1

E N D
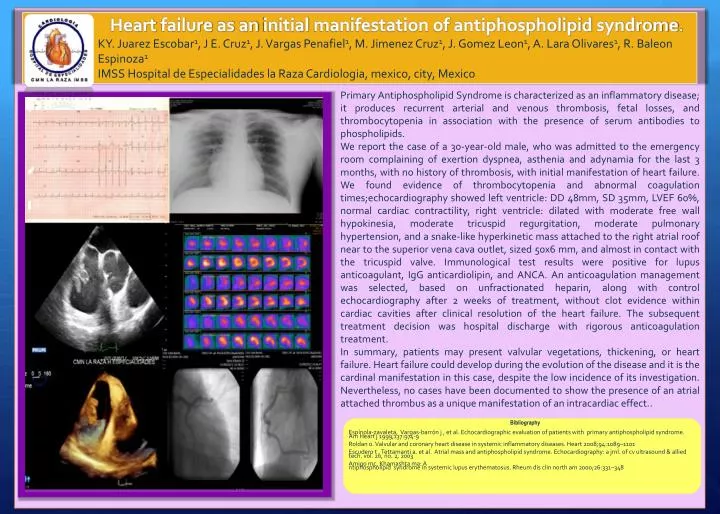
Heartfailure as aninitialmanifestation of antiphospholipidsyndrome. KY. Juarez Escobar1, J E. Cruz1, J. Vargas Penafiel1, M. Jimenez Cruz1, J. Gomez Leon1, A. Lara Olivares1, R. BaleonEspinoza1 IMSS Hospital de Especialidades la Raza Cardiologia, mexico, city, Mexico PrimaryAntiphospholipidSyndromeischaracterized as aninflammatorydisease; it produces recurrent arterial and venousthrombosis, fetal losses, and thrombocytopenia in associationwiththepresence of serumantibodiestophospholipids. Wereportthe case of a 30-year-old male, whowasadmittedtotheemergencyroomcomplaining of exertiondyspnea, asthenia and adynamiaforthelast 3 months, with no history of thrombosis, withinitialmanifestation of heartfailure. Wefoundevidence of thrombocytopenia and abnormalcoagulationtimes;echocardiographyshowedleftventricle: DD 48mm, SD 35mm, LVEF 60%, normal cardiaccontractility, rightventricle: dilatedwithmoderate free wallhypokinesia, moderatetricuspidregurgitation, moderatepulmonaryhypertension, and a snake-likehyperkineticmassattachedtotheright atrial roofneartothe superior vena cava outlet, sized 50x6 mm, and almost in contactwiththetricuspidvalve. Immunological test resultswere positive for lupus anticoagulant, IgG anticardiolipin, and ANCA. Ananticoagulationmanagementwasselected, basedonunfractionatedheparin, alongwith control echocardiographyafter 2 weeks of treatment, withoutclotevidencewithincardiaccavitiesafterclinicalresolution of theheartfailure. Thesubsequenttreatmentdecisionwas hospital dischargewithrigorousanticoagulationtreatment. In summary, patientsmaypresent valvular vegetations, thickening, orheartfailure. Heartfailurecoulddevelopduringtheevolution of thedisease and itisthe cardinal manifestation in this case, despitethelowincidence of itsinvestigation. Nevertheless, no cases havebeendocumentedto show thepresence of an atrial attachedthrombus as a uniquemanifestation of anintracardiaceffect.. Bibliography Espínola-zavaleta, Vargas-barrón j , et al. Echocardiographic evaluation of patients with primary antiphospholipidsyndrome. Am Heart j 1999;137:974-9 Roldan o. Valvularand coronary heart disease in systemic inflammatorydiseases. Heart 2008;94:1089–1101 Escuderot , Tettamantia. et al. Atrial mass and antiphospholipidsyndrome. Echocardiography: a jrnl. of cv ultrasound & allied tech. vol. 20, no. 2, 2003 Amigo mc, Khamashtama: A ntiphospholipidsyndrome in systemic lupus erythematosus. Rheum dis clin north am 2000;26:331–348