Download
1 / 31
310 likes | 438 Views
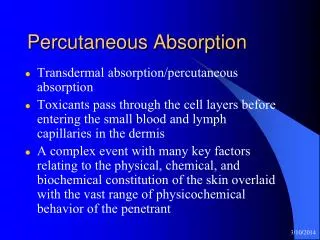
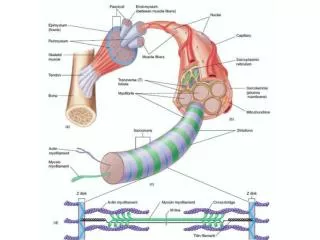
Got Filaments?..... Think. systemic lupus erythematosus (SLE) ( esp for young, black female with malar rash): “Any joint pain? other autoimmune diseases: rheumatoid arthritis (RA). Reasons why auto immune disease is important to O.D.’s. 3 rd most prevalent diseases after? cancer

E N D
Got Filaments?.....Think • systemic lupus erythematosus (SLE) (esp for young, black female with malar rash): “Any joint pain? • other autoimmune diseases: rheumatoid arthritis (RA)
Reasons why auto immune disease is important to O.D.’s • 3rd most prevalent diseases after? • cancer • heart disease • Leading cause of death/disability in women • Ocular side effects of disease • Ocular side effects of medication used for treatment
Risk Factors for autoimmune disease • female sex • increasing age • overlap (10% with Type I DM have other autoimmune disease) • familial
O.D.’s concerns for autoimmune diseases • ocular side effects of autoimmune disease • ocular side effects of medications used to treat autoimmune disease • These points were emphasized at least 4 times during lecture!
Name the two antimalarial agents that are commonly used to treat autoimmune diseases. (in order of toxicity to the eye) • Aralen® (chloroquine) • > 250mg QD • Plaquenil® (hydroxychloroquine) • > 400 mg QD • Early detection ESSENTIAL;complete patient history crucial!
Describe early & later maculopathy from antimalarial agent usage: • Early • pigment stippling • mottling • loss of FLR • Later • Central granular hyperpigmentation with surrounding zones of depigmentation and hyperpigmentation • “Bulls-Eye” maculopathy • Usually bilateral
Differential diagnosis for maculopathy from antimalarial agents • Stargardt’s • dominant cone dystrophy • Resolved central serous chorioretinopathy (CSC) • ARMD
“For Boards” • “If it looks like a bulls eye, it probably is a bulls eye • Other clues: • Aralen® (chloroquine)/Plaquenil® (hydroxychloroquine) use above 250mg/400mg qd • Aralen® (chloroquine)/Plaquenil® (hydroxychloroquine) use for more than 10 years • bilateral presentation • Remember: • Once the macula looks like this, the dammage is permanent!
Reasons why maculopathy occurs from antimalaria agent usage • long half-lives of Aralen® (chloroquine) & Plaquenil® (hydroxychloroquine) • bind with RPE melanin • interference with RPE function • decreased photoreceptors, RPE migration
prognosis of retinal toxicity effects of antimalarial agents • excellent, if antimalarial agent halted early • “bull’s eye” pattern: irreversible and advanced dammage
“Take home” risk factors for maculopathy from antimalarial agents • Aralen® (chloroquine) dosage greater than 250 mg per day • Plaquenil® (hydroxychloroquine) dosage greater than 400 mg per day • more commonly used! • on medication (@ normal dosages) more than 10 years • patients with renal insufficiency taking smaller doses • Always ask if pt has kidney problems in history!
O.D. clinical management: antimalarialmaculopathy • Standard of Care: • Baseline Exam: good history including medications, dosages & duration of use • (red?) Amsler grid: monitor for paracentralscotoma • Humphrey 10-2 perimetry (possibly with red target) • retina exam with photography • Other items: • EOG • F-100 • FlAN • OCT
Follow-up care for antimalarialmaculopathy • if no problems • follow-up at 12 months • if reproducible scotoma or macular pigment changes • PCP notified of abnormal ocular findings • PCP and patient determine whether Rx change is indicated • follow-up at 3-6 months.
the most common condition for which Plaquenil® (hydroxychloroquine) is prescribed: • SLE: systemic lupus erythematosus • Others include: • rheumatoid arthritis (RA) • discoid lupus erythematosus • Sjogren’s syndrome • sarcoidosis
“For boards” • What is this a picture illustrating? • What other ocular condition might be associated with this? • chest xray of patient with sarcoidosis. • These patients may be taking Aralen® (chloroquine) or Plaquenil® (hydroxychloroquine). • Our biggest concern is retinal toxicity from the drugs • Other ocular signs may include chronic iritis.
other medications a patient with autoimmune disease may be on that can cause ocular side effects • (oral steroids) • higher risk of posterior subcapsular cataracts (PSCs) than topical • risk of elevating IOP (topical corticosteroids usually greater risk than oral)
Young African-American Female with Malar Rash?.....Think systemic lupus erythematosus (SLE)
“For Boards”—info about diagnosing systemic lupus erythematosus • classic autoimmune disease • anti-nuclear antibodies (ANAs) always present • ANA diagnostic testing is sensitive (for autoimmune disease), but it is not specificfor a particular disease. • Symptoms: chronic & variable • joints (#1 organ involved) • kidneys • skin • febrile
systemic lupus erythematosus (SLE) epidemiology: • young, black female adults • 1.4 million Americans • Also more common in Hispanic, Asian, and Native American women
Course of systemic lupus erythematosus: • variable & unpredictable • flare-ups & remissions over many years • can be fatal (15-20%); concomitant infections, renal failure, CNS disease • not curable; with early diagnosis and treatment, most lead healthy life • 20% are disabled
treatment of systemic lupus erythematosus: • treatment outlook increasingly favorable • antimalarials • Plaquenil® (hydroxychloroquine) • NSAIDs • corticosteroids • immunosuppressants
ophthalmic manifestations of systemic lupus erythmatosus: • keratoconjunctivitissicca (most common) • retinal involvement (parallels systemic course): cotton wool spots, hemorrhages • management: steroids, immunosuppressants, laser photocoagulation • episcleritis/scleritis • management: standard treatment with adequate systemic control • uveitis?
“Boards like for you to know” diagnostic points for thyroid disease • For Graves disease: • AI complexes mimic TSH. • Recall: Normally, T3 & T4 blood levels are monitored by hypothalamus & pituitary gland. As T3T4 go up, TRH & TSH levels go down, thyroid stimulation removed T3T4 production reduced, thus keeping T3T4 at a steady-state. • In Graves disease, autoimmune complexes mimic TSH, so blood T3T4 levels are elevated, while TRH and TSH hormones are lower than normal. The normal steady-state does not occur, and hyperthyroidism is the result.
What is ‘Uhthoff’s sign’, and what systemic disease is it associated with? • blurred vision when the body gets overheated from exercise, hot weather, fever, saunas, hot tubs, or any other source of heat • multiple sclerosis
ocular manifestations of multiple sclerosis • optic neuritis (retro bulbar) • “The doctor sees nothing (abnormal)” • but, “The patient sees nothing” • 75% of patients, up to 25% initially • Visual prognosis is good • usually returns
optometric management of multiple sclerosis • follow-up within a month, including visual field • every 3-6 months thereafter
autoimmune disease (after lupus) to know • rheumatoid arthritis • chronic • systemic • autoimmune • inflammatory • more serious; causes more eye side effects
rheumatoid arthritis vs. osteo arthritis • RA: • causes more systemic symptoms; patients are sicker • osteo patients’ symptoms are relieved with sleep; RA patent’s aren’t. • RA is generally symmetrical; osteo is not.
rheumatoid arthritis treatment (ophthalmic considerations) • Plaquenil® (hydroxychloroquine) • prednisone • (same ocular considerations as SLE therapy)
The “mackdaddy” of dry eye • Sjogren’s Syndrome • post menopausal women with dry eyes & sicca complex (dry mouth, nose, vagina) • can be primary (no collagen vascular disease) or secondary to other autoimmune disease • insidious • autoimmune lymphocyte /plasma cell infiltration/destruction of lacrimal and salivary glands. viral trigger, loss of testosterone
Sjogren’s syndrome treatment: • standard: • tears • ointments • punctal plugs or cautery • filamentary keratitis: • topical steroids • acetylcysteine (*know for boards*; Dr. Landgraf has never Rx’ed) • NaCl 5% • bandage soft CL • physical removal with forceps