Download
1 / 56
560 likes | 831 Views
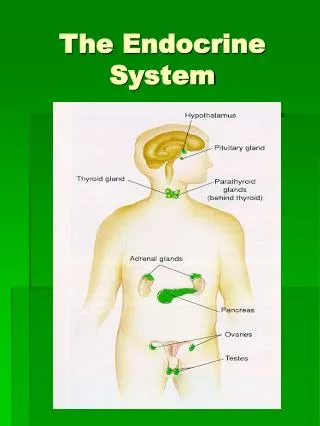
The endocrine system. Pituitary gland. Anterior lobe Posterior lobe Endocrine abnormalities Local mass effect. Hyperpituarism. Caused by adenomas: Growth hormone Adrenocorticotropic hormone Prolactin Rare – thyroid stimulating hormone, gonadortropin

E N D
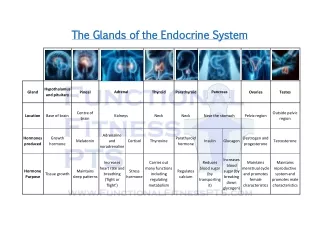
Pituitary gland • Anterior lobe • Posterior lobe • Endocrine abnormalities • Local mass effect
Hyperpituarism Caused by adenomas: • Growth hormone • Adrenocorticotropic hormone • Prolactin • Rare – thyroid stimulating hormone, gonadortropin • 25% adenomas – non-functional (causes HYPOpituarism by compression) • Microadenomas, macroadenomas (10mm) • Nuclear atypia is NOT sign of malignancy • Ultrastructurally – secretory granules
Somatotropic adenomas • Acromegaly – in adults • Gigantism – prior to closure of epiphyses • Granulated, eosinophilic cells – eosinophilic adenoma
Prolactinomas • Hypogonadism • Galactorrhea • Granulated acidophilic or chromophobic cells – chromophobicadenoma
Corticotroph tumors • Cushing’s syndrome • Basophilic cells – basophilic adenoma
Hypopituarism Caused by 1) hypothalamic lesions: • Craniopharyngioma • Glioma • Germinoma 2) pituitary lesions: • Nonsecretory adenomas • Sheehan’s syndrome • Empty sella syndrome Clinically – variable • Hypogonadotropism • Hypothyroidism, etc.
Hypothalamic lesions – craniopharyngioma • Benign cystic tumor • Calcifications • Squamous epithelial cells and reticular stroma
Nonsecretory chromophobe pituitary adenoma • Mass effect (visual problems, headache) • Chromophobic or oncocytic forms exists
Sheehan’s syndrome • Associated with obstetric haemorrhage or shock • Caused by infarction of anterior pituitary • Gonadal failure – inability to lactate • ACTH, TSH deficiency • Healing of necrosis – fibrous tissue
Posterior pituitary syndrome • Excess or deficiency of antidiuretic hormone – ADH • Caused by suprasellar/hypothalamic lesions
Posterior pituitary syndrome Excess of ADH • Abnormal resorption of water, hyponatremia and inability to excrete diluted urine Caused by ectopic ADH secretion: • Non-endocrine neoplasms (small cell carcinoma of the lung) • Non-neoplastic pulmonary diseases (TBC, pneumonia) • Primary CNS lesions (infarcts, meningitis, haemorrhage)
Posterior pituitary syndrome ADH deficiency (Diabetes insipidus) Inability to concentrate urine: • Polyuria • Polydipsia • Hypernatremia
Thyroid gland • Hyperthyroidism • Hypothyroidism • Goitre – focal, diffuse
Hyperthyroidism (thyrotoxicosis) • Increased levels of triodothyronine (T3), thyroxine (T4) • Clinically: wide-eyed gaze, tachycardia, palpitations, nervouseness, weight loss (increased appetite), moist hand, tremor, peripheral vasodilatation • Associated with diffuse hyperplasia (Graves’ disease) or with toxic multinodular goitre or toxic adenoma • May be associated with struma ovarii (teratoma)!!
Graves’ disease • Autoimmune process • Presence of thyroid stimulating antibody (TSAb) and thyrotropin binding inhibitor immunoglobulin (TBII) • Associated with other autoimmune diseases • Presence of hyperplasia of foIlicular epithelium , depletion of colloid and lymphoid aggregates
Hypothyroidism Cretinism (during infancy) • Endemic form • Sporadic form • Physical an mental retardation Myxoedema (in adults) Slowing of physical and mental activity, fatigue and apathy Signs - periorbital oedema, coarsening of skin, cardiomegaly, accumulation of mucopolysaccharides in dermis Various causes - idiopathic primary, inflammation – Hashimoto thyroiditis, etc.
Thyroiditis • Hashimoto’s thyroiditis • De Quervain’s thyroiditis • Riedel’s fibrosing thyroiditis • Lymphocytic thyroiditis • Infectious thyroiditis
Hashimoto’s thyroiditis • Autoimmune disorder • Female predominance • Defect in suppressor T cells, production of autoantibodies • Associated with other autoimmune disease (SLE, Sjögren sy, rheumatoid arthritis…) • Microscopically – dense lymphocytic infiltrate, germinal centers, abundant eosinophilic oncocytes (Hürtle cells)
De Quervain’s subacute granulomatous thyroiditis • Also known as giant cell thyroiditis • Probably viral etiology • Destruction of follicles, neutrophil infiltrate, multinucleate giant cells • Recovery in 6-8 weeks
Subacute lymphocytic thyroiditis • Nonspecific lymphoid infiltration • Without germinal centre • In women in postpartum period
Riedel’s fibrosing thyroiditis • Thyroid replaced by fibrous tissue • Fibrous tissue extends and penetrate into the surrounding neck structures • May be mistaken for infiltrating neoplasm
Tumors Benign – adenomas • Well demarcated • Fibrosis • Haemorrhage • Calcifications • Hürtle cell adenoma - oncocytic • Usually „cold“ Malignant - carcinomas • See transparency
Parathyroid gland Primary hyperparathyroidism • Hypersecretion of parathormone • Caused by adenoma (80%), hyperplasia (15%), carcinoma (5%) • Bone resorption, hypercalcemia – osteoporosis, muscle weaknes, nephrolithiasis, ulcers, pancreatitis, headache, depression Secondary hyperparathyroidism • In patients with renal failure • Compensatory hypersecretion of parathormone (reaction to phosphate retention and hypocalcemia)
Parathyroid gland - tumors Adenoma • Solitary, encapsulated – compression of adjacent gland • No stromal fat • Composed predominatly of chief cells • Part of MEN I, MEN II Carcinoma • Rare • Invasion, metastases Hyperplasia • All glands • Fat cells interspersed
Hypoparathyroidism, pseudohypoparathyroidism Hypoparathyroidism • Multiple etiology (surgical removal, autoimunne destruction, congenital…) • Tetany, neuromuscular excitability, paraesthesiae psychosis Pseudohypoparathyroidism • Rare • Abnormality PTH receptors, loss of responsiveness, hypocalcemia • Compensatory parathyroid hyperfunction
Adrenal cortex - hyperfunction Three syndromes: • Cushing’s syndrome • Hyperaldosteronism • Adrenogenital syndromes
Cushing’s syndrome Causes: • Administration of exogenous glucocorticoids – most common • Pituitary hypersecretion of ACTH (Cushing’s disease) – adenoma • Ectopic ACTH secretion – small cell carcinoma !! Histology: • Crooke’s hyaline changes within pituitary basophils Clinically: • Central obesity, moon facies, fatigability, hirsutism, hypertension, osteoporosis, cutaneous striae
Hyperaldosteronism Conn’s syndrome: • Adenoma/hyperplasia • Excessive production of aldosterone – low plasma renin, sodium retention, hypertension, loss of potassium, muscular weakness, cardiac arrhytmias, metabolic alkalosis, tetany Secondary: • Reduced glomerular perfusion (fail in blood volume) – activation of renin angiotensin system – stimulation of aldosterone secretion • Most common
Adrenogenital syndromes • Variable manifestation (virilization, pubertax praecox, hermaphroditism, pseudohermaphroditism) • Autosomal recessive trait • Most often – deficiency of 21-hydroxylase - virilization
Hypofunction of adrenal cortex • Adrenal crisis • Addison’s disease • Secondary insufficiency
Primary acute adrenocortical insufficiency • Rapid withdrawal of steroids • Massive destruction of steroids – Waterhouse-Friderichsen syndrome: • During septic meningococcal infection • Massive hemorrhage • Hypotension • Shock • DIC
Addison’s disease (chronic adrenocortical insufficiency) • Autoimunne • Infection (TBC, fungi, etc.) • Metastatic cancer (lung, stomach, etc.) • Clinically: • Anorexia • Weakness • Cutaneous hyperpigmentation • ACTH elevation (in primary insufficiency) Secondary insufficiency • decreased production of ACTH, absence of hyperpigmentation, normal aldosterone levels