Download
1 / 45
450 likes | 648 Views
Evidence based cure of Psoriasis cases . Prof G R Mohan MD(Hom),PG Dip(Env Stud) Principal, Devs Homoeopathic Medical College, drmohangr@yahoo.co.in www.drgrmohan.c. Skin disease infrequently kills, But Often produces unhappiness, Usually loss of work and social

E N D
Evidence based cure of Psoriasis cases Prof G R Mohan MD(Hom),PG Dip(Env Stud) Principal, Devs Homoeopathic Medical College, drmohangr@yahoo.co.in www.drgrmohan.c Prof G R Mohan
Skin disease infrequently kills, But Often produces unhappiness, Usually loss of work and social Deprivation as well as considerable Physical discomfort. Prof G R Mohan
Physician should know what not to do in treating skin diseases is an important thing to know. Prof G R Mohan
Concentration comes out of a combination of confidence and hunger -- Arnold palmer Prof G R Mohan
Hahnemann's rule to treat the totality of symptoms complained of by the patient, the only method by which we may cure our patients. Prof G R Mohan
How patients come to us • Skin eruption that has been for years with Cortisone used suppressed eruptions. • Eruptions cured earlier and suffering from various other problems. Prof G R Mohan
If Skin eruption that has been for years and suppressed with Cortisones Prescribe best indicated remedy based on the generals, mental emotional and on skin problems. Prof G R Mohan
If Eruptions cured earlier and suffering from various other problems If eruptions are treated, there will be problems • The organism should be stimulated by right remedy to evoke a skin eruptions Prof G R Mohan
Body must be left to fight the eruptions it self. How long to leave the eruption ? It depends up on the severity. If treated earlier for cosmetic reasons or itching The case will be spoiled . Case will be partially suppressed with half the eruption being driven inside and other half reaming on the skin Prof G R Mohan
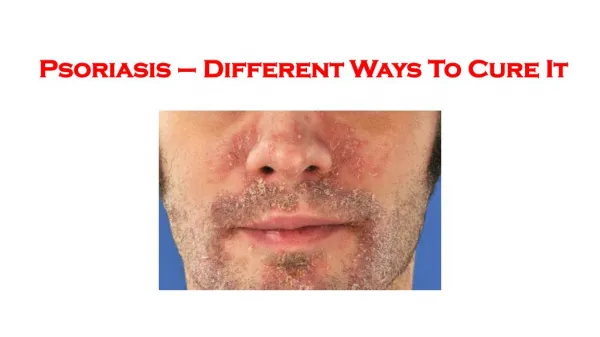
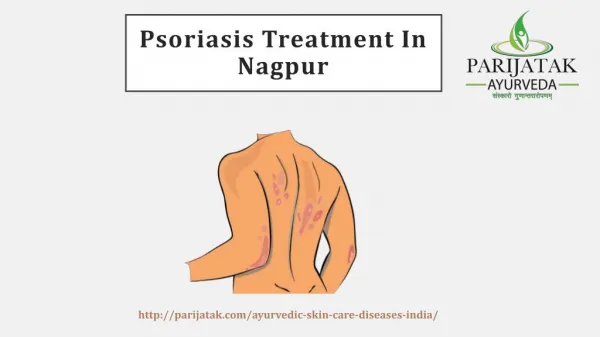
Psoriasis Psoriasis is a common , genetically determined, inflammatory skin disorder of unknown cause which in its most usual from is characterized by well-demarcated raised red scaling patches that preferentially localize to the extensor surface. Prof G R Mohan
Pathophysiology • The keratinocytes hyper proliferation due to excessive division of cells in the basal layers. • Epidermis and dermis are involved Hyperkinetic with increased cell production of new cells 20-30 times, Increased epidermal volume, Rate of nail growth increased, Formation of abnormal nucleated ,loose scaly stratum cornea. Prof G R Mohan
PSORIASIS Occurs in 1% to 2% population. Affects males( more) Age on set: early : 16-22y late : 55-60y Prof G R Mohan
Aetiology • The cause is unclear but involves immune stimulation of epidermal keratinocytes; T cells seem to play a central role. Family history is common, and certain genes and HLA antigens (Cw6, B13, B17) are associated with psoriasis. An environmental trigger is thought to evoke an inflammatory response and subsequent hyperproliferation of keratinocytes. Prof G R Mohan
Basic defects • Genetic • Bio chemical • Immunological Prof G R Mohan
Precipitating factors • Trauma • Infection • Sun light • Emotion • season Prof G R Mohan
Discoid Guttate Napkin Flexural Rupioid Pustule Nail Clinical patterns Prof G R Mohan
PSORIASIS Prof G R Mohan
Psoriasis-sites • Extensor aspects of trunk& limbs • Knees, elbows & scalp • Mucosa seem spared • Nails • Flexural areas (genital, axillae, Inframamary folds, abdominal folds, umbilicus. • Face • Site of minor injury. Prof G R Mohan
Clinical features • common, chronic, and recurrent • Very demarcated margin (plaque) • Papulo -squamus disorder. • dry ,well circumscribed, silvery, scaly papules &plaques of various sizes Prof G R Mohan
SYMPTOMS & SIGNS Gradual onset, Remitting &relapsing. Usually non itchy Horny layers Increased epidermis thickening. Prof G R Mohan
These cycles of flare-ups and remissions often lead to feelings of sadness, despair, guilt and anger as well as low self-esteem. Depression is higher in people who have psoriasis than in the general population. Feelings of embarrassment also are common. Prof G R Mohan
Severity of psoriasis • Psoriasis is graded as mild (affecting less than 3% of the body); • moderate (affecting 3-10% of the body) or severe several scales exist. Prof G R Mohan
Psoriasis Area Severity Index (PASI) • The Psoriasis Area Severity Index(PASI) is the most widely used measurement tool for psoriasis. PASI combines the assessment of the severity of lesions and the area affected into a single score in the range 0 (no disease) to 72 (maximal disease).3 Prof G R Mohan
Diagnosis • Clinical evaluation • Rarely, biopsy Prof G R Mohan
Patient Ms T, aged 33y,house wife, came (03/01/2009)with eruptions over ears, scalp, hands ,Weight 47 Kgs, hand s, scalp, neck ,hairline margin with itching, thirst less, Case was Diagnosed as Psoriasis by local dermatologist. F/H : DM & HTN Prof G R Mohan
The case was repertorised by Phataks method Reportorial analysis is : Graphites 20/2, Pulsatilla 20/2, sepia 21/2, 3/01/09 : eruption over ears, scalp, hands with itching ,sadness, Pulsatilla was selected giving importance to Thirst less ,aversion to water Pulsatilla 30,3 doses were given placebo for 30 days, advice about diet was given. 06/02/09 – eruption increased with itching, oozing was present, Graphites 30,3 doses, Placebo for 15 days, advice about diet and personal cleanliness was given. Prof G R Mohan
21/05/09 Prof G R Mohan
21/05/09 Due domestic problems she came late for one month and half she was better and again itching, oozing started in the same places, Graphites 30,3 doses, Placebo for 15 days, 30/07/09 oozing is lees ,itching is less ,sadness still persisting Graphites 200,3 doses, Placebo for 30days were given. Prof G R Mohan
03/08/09 no oozing ,itching is less ,sadness is less ,scalp still scales are seen, hair fall still persisting, Graphites 200,3 doses, Placebo for 30days were given. Prof G R Mohan
03/8/2009 Prof G R Mohan
03/08/09 Prof G R Mohan
30/10/09 30/10/09 no oozing , occasional itching ,sadness is less ,scalp scales are few seen, hair fall better , Placebo for 30days were given. Prof G R Mohan
30/10/09 Prof G R Mohan
24/11/09 : itching increased, Graphites IM,1doses,Placebo for 30days were given 25/12/09 skin totally cleared from eruptions, Placebo for 30days was given Prof G R Mohan
29/6/10 29/06/2010 she came after 6 months after stopping medication (as shown in visual ) Prof G R Mohan
Patient Mr. A, aged 30y,Software eng, came (21/01/09)with fissures over tongue since 3years diagnosed as Psoriasis of tongue by Dermatologist. , sleeplessness, Weight 53 Kgs, thirst less,
Case no 2 Patient Mr. A, aged 30y,Software eng, came (21/01/09)with fissures over tongue since 3years diagnosed as Psoriasis of tongue by Dermatologist, sleeplessness, Weight 53 Kgs, thirst less, Prof G R Mohan
21/01/09 itching increased, Acid Nitricum 30c ,5 doses, Placebo for 30days were given 5/03/09 no change no difference in taste , sleeplessness . Acid Nitricum 30c , Placebo for 30days were given 16/08/09 patient is feeling fissures are reducing , no difference in taste , sleeplessness is better, Acid Nitricum 200c, 3 doses, Placebo for 30days were given. 19/09/09 fissures are reducing , no difference in taste , sleeplessness is better, Acid Nitricum 200c, 3 doses, Placebo for 30days were given. 23/10/09 : had fever a month back was admitted in hospital took allopathic medicines, fissures are reducing, Ars Alb 200c,( because he was still felling after affects of fever) 3doses, Placebo for 30days were given. 29/12/09 no change , Thuja 1m I dose was given, Placebo for 30days were given
21/02/10 anterior part of tongue improved a lot as shown in visual, thickness of tongue reduced a lot , Acid Nitricum IM, 1doses, Placebo for 30days were given.
Views of authors about psoriasis of tongue They report that fissured tongue (FT) and benign migratory glossitis (BMG; geographic tongue) were the two most frequent findings. FT affected 33% of psoriasis patients and 9.5% of controls, while BMG affected 14% of patients and only 6% of controls. Notably, the frequency of BMG increased with the severity of psoriasis in a sub-group of patients with plaque-type disease, as assessed by Psoriasis Area and Severity Index, Daneshpazhooh et al report in the journal BMC Dermatology. They conclude: "Overall, although oral lesions might not be considered authentic oral psoriasis unless proven histologically and with a parallel clinical course, nonspecific tongue lesions are significantly more frequent in psoriatic cases." The team recommends further studies to "evaluate the clinical significance of these seemingly nonspecific lesions in a suspected psoriatic case". Tongue lesions common in psoriasis patients 12 November 2004 BMC Dermatol 2004; 4: 16. http://www.medwire-news.md/60/30030/Psoriasis/Tongue_lesions_common_in_psoriasis_patients.html
Conclusion Skin disease infrequently kills, But Often produces unhappiness, Usually loss of work and social Deprivation as well as considerablePhysical discomfort. has proved to be correct in both cases. Concentration to treat comes out of a combination of confidence in system and hunger to learn is a fact. Prof G R Mohan
References • Marks. R, Roxburgh’s Common Skin Diseases, 16th Edition, Chapman & Hall Medical, London [page no.124-140] • Behl. P.N., Practice of Dermatology, Eighth Edition, CBS Publishers & Distributors, New Delhi, India [page no.253-260] • http://psoriasis,about.com/od/psoriasisfags/f/pasi.htm Prof G R Mohan