Download
1 / 35
350 likes | 542 Views
Medical Treatment for Atrial Fibrillation Prevention Role of Renin – Angiotensin Antagonists Dr. V. Witzling. Prevalence of Atrial Fibrillation In general population. Atrial fibrillation : Paroxysmal Persistent Chronic. Goals of treatment : Prevention

E N D
Medical Treatment for Atrial Fibrillation Prevention Role of Renin – Angiotensin Antagonists Dr. V. Witzling
Prevalence of Atrial Fibrillation In general population
Atrial fibrillation: • Paroxysmal • Persistent • Chronic
Goals of treatment : • Prevention • Reduce the risk of thromboembolism • Control symptoms : • Rate control • Rhythm control
Treatment : • Acute management : • Electrical cardioversion • Chemical cardioversion • Rate control
Long term management : • Rate control • Drugs • AV nodal ablation and permanent pacing • Rhythm control • Drugs • Catheter ablation • Maze procedure
Current treatment strategies are far from optimal • Anticoagulation - expensive and has its risk • Anti-arrhythmic drugs – imperfect and with side effects • Ablation – complex and with potential for major complications
Safety issues – ablation • Pulmonary Vein Stenosis • Cerebrovascular accident (CVA) • Bezold-Jarisch response (?RSPV) • Phrenic nerve injury (RSPV) • Cardiac tamponade • Pulmonary parenchymal hemorrhage and bronchial vein damage • Atrioesophageal fistula formation
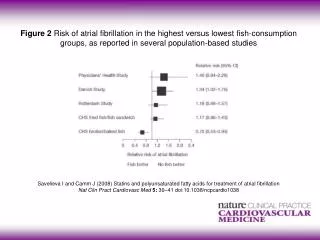
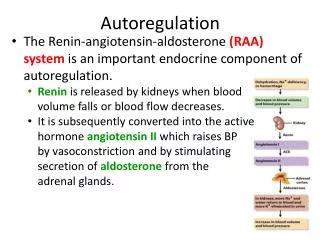
Evidence of the importance of the RAAS for cardiovascular disease is partly attributable to the finding that : • renin activity predicts cardiovascular events • Inhibition of the system improves cardiovascular morbidity and mortality • ACEI’s and ARBs
New research direction • to target the atrial fibrillation substrate • to examine if drugs can produce atrial structural and electrical remodeling • whether this results in clinically significant reduction of atrial fibrillation burden
Relation RAAS – AF : • Studies in various patient populations with AF as secondary end point • Hypertentsion • Congestive heart failure • Post myocardial infarction
Hypertension – LIFE study • > 9000 patients with hypertension and LVH by ECG • Losartan vs. Atenolol • Primary endpoint ( death,MI and stroke ) significantly reduced in the losartan arm
Heart Failure – Val-HeFT study • > 5000 patients, in NYHA class II-IV and with a LVEF < 40% • Valsartan vs. placebo • Significant reduction of combined mortality and morbidity from heart failure in the valsartan arm
Post MI – TRACE study • > 1700 patients, 2 to 6 days after MI, with LVEF≤35% • Trandolapril vs. placebo • Primary endpoint ( death ) reduced significantly in the trandolapril arm
Clinical trials with AF as primary end point: • Madrid • Ueng
Conclusion • The initial basic science and clinical trial data suggests that modulation of the RAS system may be a treatment for preventing atrial fibrillation • Points to be clarified : • Do these drugs have a clinically meaningful impact on atrial fibrillation? • If there is an impact, is it similar in all atrial fibrillation patients? • Do ACEI’s and ARBs have similar benefits?
Conclusion • Currently there is no enough data to recommend the use of ACEI’s and ARBs in routine clinical practice for prevention of atrial fibrillation. • Sufficient data for the European Society of Hypertension and the European Society of Cardiology to recommend ACEI or ARB first line treatment for hypertensive patients that also have recurrent PAF ( guidelines for hypertension 2007)